Ultrasound-Guided Neuroma Injection
Author
Shankar Hariharan, MD
Associate Professor
Department of Anesthesiology
Medical College of Wisconsin and Zablocki VA Medical Center
Milwaukee, WI
Commentary
Bernhard Moriggl, MD
Professor
University of Innsbruck
Innsbruck, Austria
Introduction
Neuromas occur following varying degrees of nerve injury anywhere in the body. They are part of the reparative process and the appearance is dictated by the availability of a distal tract or Schwann cell. Sometimes the site of the neuroma can be a source of pain. With residual limb pain, the cause of pain may be due to scar tissue producing traction on the nerve and neuroma, from compression by the adjacent tissues or vessels or from ischemia due to decrease in blood supply.[1-2] Managing pain arising from the neuroma is challenging. The treatment options include injection of local anesthetic, steroid and neurolytic agents, cryo-ablation, radiofrequency ablations and surgical revision.[3-7] Unfortunately modifying the surgical technique to prevent neuroma formation has not always been successful.[8]
Anatomy
There are two major categories of neuromas based on their appearance. Spindle neuromas occur as fusiform swelling following micro-trauma due to friction or irritation to the nerve, not enough to disrupt the trunk. Terminal neuromas occur following severe trauma leading to avulsion, surgical or traumatic sectioning of the nerves. The size of the neuromas depend on the initial size of the nerve, number of injured axons, recurrent trauma or irritation, the environment and rate of growth. The typical time frame for the formation of a neuroma is about 6-8 weeks. Neuromas typically stop their growth after a year.
Morton’s neuroma was initially described by Civinini in 1835 and followed by a series in 1876 by Morton. The prevalence rate of Morton’s neuroma is 30–33%.[9] It is an inter-digital neuroma arising from the plantar digital nerve commonly between the 2–3rd and 3–4th inter-metatarsal spaces. Although some authors would argue that it is not a true neuroma, it has similar sonographic appearance and is known to cause forefoot pain and paraesthesia. It lies beneath the interosseous muscle in a common sheath with the artery and the inter-metatarsal ligament is just proximal to it.[10] The digital nerve from which it arises is about 2 mm in diameter and is rarely visualized. Excessive pronation and cavus feet are thought to be the predisposing factors.4 The size of the Morton’s neuroma is usually around 5 mm although sizes up to 20 mm have been described.[11]
Sonographic evaluation of neuromas has been documented since the 1990s.[12-16] The success in identifying the neuroma ranges from 85–100%.[14][17-19] Neuromas in other locations including the bile duct have also been documented.20 In a prospective study of 73 patients with clinical symptoms of Morton’s neuromas, sonography was performed for diagnosis which was subsequently confirmed in 95% based on surgical and pathological findings. The average size of the neuromas was 6.2 mm.[12] Ultrasound detection of Morton’s neuroma was successfully confirmed by MRI in 79% of the cases. The authors comment that operator dependency of the technique and the size of the lesion are likely responsible for the lower rates of detection by ultrasound compared to earlier reports.[21]
Neuroma appears as an incompressible, oval, bulbous, hypo-echoic structure in continuity with the nerve. Sometimes hyperechoic bands representing intraneural connective tissue are also seen. The margins may be well defined or irregular. Anecdotal report of vascularity changes in tissues surrounding a neuroma has been described.2
Traditional Technique
Most pain medicine practitioners perform blind targeting of the area of pain in the possible location of the neuroma. When performing the procedure blind, “diagnostic injections” with local anesthetic may not be accurate thus may have missed the nerve or the injection may be intravascular by accident. Both situations will lead to a false negative response rate.
CT and MRI have been utilized for the diagnosis and targeting of neuromas.[1][22] When contrast enhancement is used with CT it is often not adequate for visualization of vascular structures unlike ultrasound.[1][22] Ultrasound guidance for the identification and specific targeting of the neuromas has been described.[5][11][23-25] For intra-neuronal injection, localizing the injectate is recommended for producing effective neurolysis.[26-27]
Ultrasound Technique
 Figure 1. Transverse sonographic view of a sciatic stump terminal neuroma appearing as a bulbous hypoechoic structure in continuity with the sciatic nerve.
Figure 1. Transverse sonographic view of a sciatic stump terminal neuroma appearing as a bulbous hypoechoic structure in continuity with the sciatic nerve.
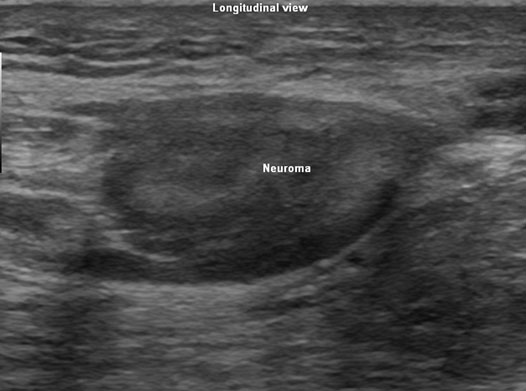 Figure 2. Longitudinal view of the sciatic terminal neuroma appearing hypoechoic.
Figure 2. Longitudinal view of the sciatic terminal neuroma appearing hypoechoic.
Ultrasound guidance for targeting these neuromas was initially described by Masala in 2001.28 Ultrasound guided steroid injection into the neuroma has become routine practice in a few centers.[5][11] Ultrasound has also been utilized for pre-procedure localization of neuromas.[25]
Depending on the location of the pain and neuroma, a scout scan is performed using a linear array transducer with appropriate frequency, usually in the range of 7–15 MHz depending on the depth of the target. The scan is performed both in the transverse and longitudinal views in the possible direction of the neuroma (Figures 1 & 2). Once the neuroma is identified the nerve is followed proximally and distally to measure the length and width of the neuroma. No scan is complete without a color flow Doppler study to identify the vessels in the neighborhood. This also facilitates in planning a needle trajectory.
The target for diagnostic local anesthetic injections is the distal end of the nerve before the neuroma. It may be approached either in plane or out of plane depending on individual preferences and familiarity with the technique. The diagnostic injection may be performed by encircling the neuroma with local anesthetic. Depending on the target the amount of local anesthetic used may vary from 1–10 mL. Once the source of pain is identified to be originating from the neuroma, neurolytic or steroid injections to the nerve may be performed subsequently by injecting into the proximal portion of the neuroma itself. If the source of pain is from the scar tissue, separation of the fibrous tissue may be performed with a larger volume of steroid injected under ultrasound guidance to the area of the scar surrounding the neuroma. The usual volume of neurolytic solution required ranges from 0.75–5 mL depending on the size and location of the neuroma. The neurolytic injections are performed following an injection of about 2–10 mL of local anesthetic to the area proximal to the neuroma on the nerve. An alternative technique to neurolysis is to perform a radiofrequency or cryo ablation under ultrasound guidance.
The complications of steroid injections are thinning of the overlying skin, and hyper pigmentation. When performing neurolytic injections, the sclerosant may cause skin necrosis.
Literature Review
Ultrasound examination of neuromas was reported as early as 1957.29 Many reports of the utility of ultrasound in diagnosing Morton’s neuroma was followed subsequently by ultrasound guided steroid and neurolytic injections. One of the earliest studies on ultrasound guided intra-lesional injection for Morton’s neuroma was performed using 30% alcohol. Of the 23 patients who received multiple injections every 7-10 days, 91% reported complete pain relief.[28] US guided alcohol injection into the Morton’s neuroma of 40 patients, using 0.5 mL of a sclerosing solution containing carbocaine and 30% ethyl alcohol, resulted in 100% technical success. The authors repeated the injections 4 times at 15-day intervals for a total of 160 injections. Partial or total pain relief was reported in 90% of the patients in 15 days.[24] In another series, 101 patients received 20% alcohol injections into the inter-digital neuromas with significant reduction in pain. There was an average of 4.1 injections done per patient. The authors’ recommendation for the use of sonography was to avoid leakage of sclerosant into the neighboring tissues. 84 of 100 patients were pain free following the injections.[30]
During a short term follow up for 7 days following a single ultrasound guided steroid (triamcinolone) injection into the inter-metatarsal neuroma of 24 patients, excellent pain relief was reported in 62% of the patients.[11] Similar results were obtained with a follow up for 9 months by another group on 35 patients.[31] In a retrospective study 28 out of 45 patients (63%) diagnosed sonographically to have Morton's neuroma achieved complete pain relief following ultrasound guided injection of 20 mg of triamcinolone acetonide. The average follow up was for 11.4 months.[32]
Gruber et al injected 10 patients with stump neuroma under ultrasound guidance using phenol. Following a diagnostic injection with local anesthetic, the patients received 0.3–1 mL of phenol intra-neuronally into the proximal portion of the neuroma. 7 patients received complete relief and the remaining 3 refused further injections. There was no change in the size of the neuroma at 1 month follow up.[7] To look at the effects of phenol injection into the neuroma under ultrasound guidance, the same authors recruited 82 patients with signs and symptoms of painful stump neuroma. Using high resolution sonography with a linear array transducer, the location of the neuromas was identified and measured. Following a diagnostic injection with local anesthetic, each patient received 0.8 mL of phenol into the neck of the neuroma under ultrasound guidance. This was repeated at 6 weeks and 12 weeks. They noticed that the maximum pain relief was obtained after the first injection. They also observed that none of the patients had residual pain after the third injection. They did not observe any significant difference in the size of the neuroma with sonography at follow up. The weakness of this study is that 30 patients were lost to follow up.[26]
More recently, ultrasound identification of neuromas were confirmed intra-operatively in 19 patients with upper limb nerve pathology. The authors used linear array transducers with frequencies in the range of 7–9 MHz.[33]
Commentary
Classification of Procedure
This is considered a basic level (1) block.
General Remarks
Accurate detection of neuromas requires proper knowledge of the peripheral nerves and their courses. Often there are valuable anatomical landmarks that help to identify the neuromas of other peripheral nerves besides Norton's neuroma. For example, anatomical landmarks that are useful for localization of the neuroma are as follows:
- the small saphenous vein helps to locate the neuroma of the sural nerve;
- the posterior tibial vessels and the flexor tendons (digitorum and hallucis) help to locate the neuroma of the tibial nerve within the tarsal tunnel;
- the anterior tibial artery helps to locate the neuroma of the deep peroneal nerve in the anterior compartment).
In the above situations, Color Doppler assessment is extremely valuable for detecting the vessels associated with the neuromas.
Finally, the surface of the distal fibula is a useful landmark that helps to locate the neuroma of the superficial peroneal nerve.
References
- Singson RD, Feldman F, Slipman CW, Gonzalez E, Rosenberg ZS, Kiernan H. Postamputation neuromas and other symptomatic stump abnormalities: Detection with CT. Radiology 1987;162:743-5.
- Shankar H. Ultrasound demonstration of vascularity changes with changes in pain perception in a stump neuroma. Clin J Pain 2009;25:253-5.
- Kirvela O, Nieminen S. Treatment of painful neuromas with neurolytic blockade. Pain 1990;41:161-5.
- Dockery GL. The treatment of inter-metatarsal neuromas with 4% alcohol sclerosing injections. J Foot Ankle Surg 1999; 38:403-8.
- Ernberg LA, Adler RS, Lane J. Ultrasound in the detection and treatment of a painful stump neuroma. Skeletal Radiol 2003;32:306-9.
- Neumann V, O'Connor RJ, Bush D. Cryoprobe treatment: An alternative to phenol injections for painful neuromas after amputation. AJR Am J Roentgenol 2008;191:W313; author reply W314.
- Gruber H, Kovacs P, Peer S, Frischhut B, Bodner G. Sonographically guided phenol injection in painful stump neuroma. AJR Am J Roentgenol 2004;182:952-4.
- Lewin-Kowalik J, Marcol W, Kotulska K, Mandera M, Klimczak A. Prevention and management of painful neuroma. Neurol Med Chir (Tokyo) 2006;46:62, 7; discussion 67-8.
- Bencardino J, Rosenberg ZS, Beltran J, Liu X, Marty-Delfaut E. Morton's neuroma: Is it always symptomatic? AJR Am J Roentgenol. 2000;175:649-53.
- Redd RA, Peters VJ, Emery SF, Branch HM, Rifkin MD. Morton neuroma: Sonographic evaluation. Radiology 1989;171:415-7.
- Sofka CM, Adler RS, Ciavarra GA, Pavlov H. Ultrasound-guided interdigital neuroma injections: Short-term clinical outcomes after a single percutaneous injection-preliminary results. HSS J 2007;3:44-9.
- Pollak RA, Bellacosa RA, Dornbluth NC, Strash WW, Devall JM. Sonographic analysis of morton's neuroma. J Foot Surg 1992;31:534-7.
- Kaminsky S, Griffin L, Milsap J, Page D. Is ultrasonography a reliable way to confirm the diagnosis of Morton’s neuroma? Orthopedics 1997; 20:37-9.
- Shapiro PP, Shapiro SL. Sonographic evaluation of interdigital neuromas. Foot Ankle Int 1995;16:604-6.
- Sobiesk GA, Wertheimer SJ, Schulz R, Dalfovo M. Sonographic evaluation of interdigital neuromas. J Foot Ankle Surg 1997;36:364-6.
- Provost N, Bonaldi VM, Sarazin L, Cho KH, Chhem RK. Amputation stump neuroma: Ultrasound features. J Clin Ultrasound 1997;25:85-9.
- Kankanala G, Jain AS. The operational characteristics of ultrasonography for the diagnosis of plantar intermetatarsal neuroma. J Foot Ankle Surg 2007;46:213-7.
- Quinn TJ, Jacobson JA, Craig JG, van Holsbeeck MT. Sonography of morton's neuromas. AJR Am J Roentgenol 2000;174:1723-8.
- Oliver TB, Beggs I. Ultrasound in the assessment of metatarsalgia: A surgical and histological correlation. Clin Radiol 1998;53:287-9.
- Shimura K, Tamada K, Asada M, Watabiki N, Wada I, Tanaka N, et al. Intraductal ultrasonography of traumatic neuroma of the bile duct. Abdom Imaging 2001;26:632-4.
- Lee MJ, Kim S, Huh YM, Song HT, Lee SA, Lee JW, et al. Morton neuroma: Evaluated with ultrasonography and MR imaging. Korean J Radiol 2007;8:148-55.
- Singson RD, Feldman F, Staron R, Fechtner D, Gonzalez E, Stein J. MRI of postamputation neuromas. Skeletal Radiol 1990;19:259-62.
- Beggs I. Sonographic appearances of nerve tumors. J Clin Ultrasound 1999;27:363-8.
- Fanucci E, Masala S, Fabiano S, Perugia D, Squillaci E, Varrucciu V, et al. Treatment of inter-metatarsal Morton’s neuroma with alcohol injection under US guide: 10-month follow-up. Eur Radiol 2004;14:514-8.
- Thomas AJ, Bull MJ, Howard AC, Saleh M. Peri operative ultrasound guided needle localisation of amputation stump neuroma. Injury 1999; 30:689-91.
- Gruber H, Glodny B, Bodner G, Kopf H, Bendix N, Galiano K, et al. Practical experience with sonographically guided phenol instillation of stump neuroma: Predictors of effects, success, and outcome. AJR Am J Roentgenol 2008;190:1263-9.
- Sung DH, Han TR, Park WH, Je Bang H, Kim JM, Chung SH, et al. Phenol block of peripheral nerve conduction: Titrating for optimum effect. Arch Phys Med Rehabil 2001;82:671-6.
- Masala S, Fanucci E, Ronconi P, Sodani G, Taormina P, Romagnoli A, et al. Treatment of intermetatarsal neuromas with alcohol injection under US guide. Radiol Med 2001;102:370-3.
- Cappellini O. Ultrasonic study of neuromas of the peripheral nerves. Chir Organi Mov 1957;45:26-33.
- Hughes RJ, Ali K, Jones H, Kendall S, Connell DA. Treatment of Morton’s neuroma with alcohol injection under sonographic guidance: Follow-up of 101 cases. AJR Am J Roentgenol 2007;188:1535-9.
- Markovic M, Crichton K, Read JW, Lam P, Slater HK. Effectiveness of ultrasound-guided corticosteroid injection in the treatment of Morton’s neuroma. Foot Ankle Int 2008;29:483-7.
- Hassouna H, Singh D, Taylor H, Johnson S. Ultrasound guided steroid injection in the treatment of interdigital neuralgia. Acta Orthop Belg 2007;73:224-9.
- Toros T, Karabay N, Ozaksar K, Sugun TS, Kayalar M, Bal E. Evaluation of peripheral nerves of the upper limb with ultrasonography: A comparison of ultrasonographic examination and the intra-operative findings. J Bone Joint Surg Br 2009;91:762-5.
Leave a commentOrder by
Newest on top Oldest on top