President's Message: ASRA Pain Medicine, Member Focused and Member Driven
Cite as: Provenzano D. President's message: ASRA Pain Medicine member focused and member driven. ASRA Pain Medicine News 2024;49. https://doi.org/10.52211/asra110124.001.
 With the 23rd Annual Pain Medicine Meeting in Las Vegas and the 50th Annual Regional Anesthesiology and Acute Pain Medicine Meeting in Orlando approaching, I’m reflecting on ASRA Pain Medicine’s ongoing strength in pain management. The society is flourishing, and the metrics show it. Our last spring meeting saw the most medical attendees since COVID-19 for the
acute pain and regional anesthesia meeting. Attendees’ feedback was also positive with one member noting, “I have been a member of ASRA for 20 years. The annual meetings have been so helpful to my practice of regional anesthesia. I
will be retiring and will miss the camaraderie of all. I have enjoyed all the friends and learning with these meetings.” The fall meeting is also thriving. With more than 500 abstracts submitted, a record number for the pain medicine meeting,
and registration numbers tracking high, we are gearing up for what is sure to be an unforgettable event.
With the 23rd Annual Pain Medicine Meeting in Las Vegas and the 50th Annual Regional Anesthesiology and Acute Pain Medicine Meeting in Orlando approaching, I’m reflecting on ASRA Pain Medicine’s ongoing strength in pain management. The society is flourishing, and the metrics show it. Our last spring meeting saw the most medical attendees since COVID-19 for the
acute pain and regional anesthesia meeting. Attendees’ feedback was also positive with one member noting, “I have been a member of ASRA for 20 years. The annual meetings have been so helpful to my practice of regional anesthesia. I
will be retiring and will miss the camaraderie of all. I have enjoyed all the friends and learning with these meetings.” The fall meeting is also thriving. With more than 500 abstracts submitted, a record number for the pain medicine meeting,
and registration numbers tracking high, we are gearing up for what is sure to be an unforgettable event.
So, where does the strength of ASRA Pain Medicine come from? Why do so many individuals elect to be part of the organization and volunteer their time? Why do so many use their talent to help the society achieve its mission of advancing the science and practice of regional anesthesia and pain medicine to improve patient outcomes through research, education, and advocacy? Having just concluded our September board meeting and reflecting on my journey with ASRA Pain Medicine, I want to share some crucial aspects of sustainability and offer a roadmap for future success.
First, the key to success lies in the passion and talent of volunteers and the dedication of the board of directors as well as the home office team. It’s a privilege to work with the 10 remarkable board members of ASRA Pain Medicine; their strength and commitment always impress me. I continuously learn from each board member. Additionally, the organization’s structure and leadership are crucial. Extensive education and exceptional mentorship prepare individuals for board roles. This has been vital for my leadership journey since I actively started getting involved in ASRA Pain Medicine after completing my fellowship at Dartmouth Hitchcock Medical Center in 2006. With the recent election of Drs. Stephen Haskins and Christine Hunt to the ASRA Pain Medicine Board (terms beginning spring 2025), the society welcomes two new enthusiastic board members who will continue to advance the field. Each will bring their unique perspective: Dr. Haskins, with his expertise in perioperative point-of-care ultrasound, and Dr. Hunt, with her physical medicine and rehabilitation background, which will foster innovation and expand what’s possible in pain. We also owe so much to past boards and executive committees that prioritized future goals, attentively listened to members, and upheld strong fiduciary responsibilities. Dr. Joseph Neal always emphasized the importance of following policies and processes, a lesson that has become even more significant to me in my current leadership role.
First, the key to success lies in the passion and talent of volunteers and the dedication of the board of directors as well as the home office team.

However, all this effort and time would be wasted if its members did not have a strong commitment to the vision and mission of ASRA Pain Medicine. Ultimately, societies exist to serve their members. The role of medical societies has been evolving, accelerated by the COVID-19 pandemic starting in 2020. At our recent board retreat in September, we evaluated our members’ needs and discussed the strengths of ASRA Pain Medicine and the areas in which we need to continue to grow. We gathered input from our membership committee and leaders. Moreover, we invited current and former members who chose not to renew their memberships to share their opinions and insights. I will summarize these discussions in three main areas: attending membership strengths and benefits, residents and fellows, and areas for future growth.

Attending Membership Strengths and Benefits
Currently, we have a strong membership portfolio that includes:
- access to Regional Anesthesia and Pain Medicine (impact factor of 5.1; 5/64 in anesthesiology);
- three podcasts (ASRA News, RAPP, and RAPM Focus);
- discounts to our two annual meetings and satellite courses (Ultrasound Guided Regional Anesthesia and Perioperative Point-of-Care Ultrasound);
- research grants (Carl Koller Memorial Research Grant, Chronic Pain Medicine Research Grant, Early-Stage Investigator Award, and Graduate Student Award);
- mentor match program;
- webinars;
- 25 special interest groups (including but not limited to Cancer Pain and Supportive Care, Cannabis in Acute and Chronic Pain, Educators in Regional Anesthesia, Green Anesthesia, Opioid Safety and Substance Use Disorder, Neuromodulation, Women in Regional Anesthesia and Pain Medicine, and Private Practice); and
- ASRA Pain Medicine News (Chair: Dr. Vivian Ip, Vice Chair and Editor: Dr. Anthony Machi, Associate Editor - Regional: Dr. Kwesi Kwofie, Associate Editor - Pain: Dr. Priyanka Singla).

Furthermore, membership dues contribute to our robust advocacy efforts, including representation at the AMA House of Delegates, Current Procedural Terminology® (CPT) Editorial Panel, and RVS Update Committee (RUC). These initiatives have significantly benefited both the acute and chronic pain management fields, as evidenced by the development of codes for fascial plane and transversus abdominis plane blocks and the submission of a category one code for percutaneous interlaminar lumbar decompression. Furthermore, we will continue to advocate with our society partners through the Pain Medicine Coalition, a national coalition advocating for responsible pain care for all patients. Additionally, we consistently release clinically relevant guidelines that are globally respected. Three guidelines were published in the last year:
- Standardizing Nomenclature in Regional Anesthesia: An ASRA-ESRA Delphi Consensus Study of Upper and Lower Limb Nerve Blocks
- Evidence-Based Clinical Practice Guidelines on Postdural Puncture Headache: A Consensus Report From a Multisociety International Working Group
- Use of Corticosteroids for Adult Chronic Pain Interventions: Sympathetic and Peripheral Nerve Blocks, Trigger Point Injections - Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, the American Society of Interventional Pain Physicians, the International Pain and Spine Intervention Society, and the North American Spine Society
There are currently three more under review (ASRA Pain Medicine Consensus Practice Infection Control Guidelines for Regional Anesthesia and Pain Medicine, Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fifth Edition), and Use and Safety of Corticosteroid Injections: Joints and Musculoskeletal Soft Tissue Injections - Guidelines from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, the American Society of Interventional Pain Physicians, the International Pain and Spine Intervention Society, and the North American Spine Society), and 10 others are in progress.
Guidelines in Progress
- Baby Steps to Mastery: Building Blocks for Novices in Pediatric Regional Anesthesia
- Gastric Ultrasound for Assessing Aspiration Risk in Complex Patients Undergoing Regional and Pain Procedures
- Safety of Steroid Injections: Neuraxial Injections and Associated Topics
- Inpatient Management of Headache Patients
- Opioid Use Disorder (OUD) in the Outpatient Setting
- ASRA/ESRA Joint Recommendations for RA Education and Training: Systematic Review
- Multi-Society Guidelines for Diagnostic and Therapeutic Occipital Nerve Block Injections
- Prevention and Management of Neurological Complications Following Regional Anesthesia from ASRA, ESRA, and LASRA
- Multi-Society Guidelines on Peripheral Nerve Stimulation for Chronic Low Back Pain
- Multi-Society Knee Osteoarthritis Radiofrequency Ablation Guidelines
When we surveyed current members about the merits of ASRA Pain Medicine, they mentioned terms like innovative, cutting-edge, trustworthy, and family atmosphere. We were glad to hear these traits and will continue to foster them. Here are some additional comments from our members: “I believe that the Society is growing and targeting the proper areas of practice as the house of medicine evolves in relation to acute/chronic pain and regional anesthesia/analgesia.” “Thank you so much! This organization has given my professional career significant meaning and purpose.”
Residents and Fellows
Another key area of our continued focus is the education of residents and fellows. They represent the future of the field, and the ASRA Pain Medicine board consistently allocates significant resources to support their leadership training and development. We continue to partner and assist the leadership of the fellowship programs through our commitment and association with the Association of Pain Program Directors (APPD) and the Regional Anesthesia Fellowship Director Association (RAFDA). Both these organizations also have direct connections to and support from the ASRA Pain Medicine Board of Directors. ASRA Pain Medicine trainee initiatives include meet and greets (in person and virtual), quiz bowls at the annual meetings, problem-based learning discussions on the website, success kit for fellows, advocacy initiatives, podcasts, special speaker series, webinars, and the resident and fellow ambassador program. The engagement from the Resident and Fellow Committee during the last several years has been incredible. The current leadership (Chair: Dr. Anishinder Parkash and Chair-Elect: Dr. Crystal Joseph) continues to foster ideas and engage the trainee membership in new ways. We also continue offering the mentor match program for trainees and practicing physicians.

It is great to hear residents and fellows from other specialties, such as physiatry, talk about the degree of engagement the society offers them. It is critical that we welcome these other specialties like physiatry, neurology, and emergency medicine into our society. The demographics of pain management are rapidly changing. In 2019, anesthesiology accounted for 67% of ERAS Fellowship applicants to pain medicine by GME residency specialty with physical medicine and rehabilitation at 19%. By 2023, anesthesiology dropped to 43%, while physiatry increased to 30%. In 2024, physical medicine and rehabilitation comprises 39% of the applicant pool, surpassing anesthesiology at 34%. (Figure 1)
Moreover, seeing recent attacks undermining pain medicine fellowship education through social media and publications is disheartening. At ASRA Pain Medicine, we value the efforts of the fellowship directors in training capable and ethical future pain physicians. Instead of criticism, we will provide resources to support and improve fellowship education. Undermining this foundation gets us nowhere. For the second year in a row, we will be offering the Advanced Interventional Pain Management Course and Workshop for fellows, led by Dr. Sayed Wahezi, as well as the Medical Education Master Class for educators, led by Dr. Trent Emerick, in conjunction with the 23rd Annual Pain Medicine meeting.
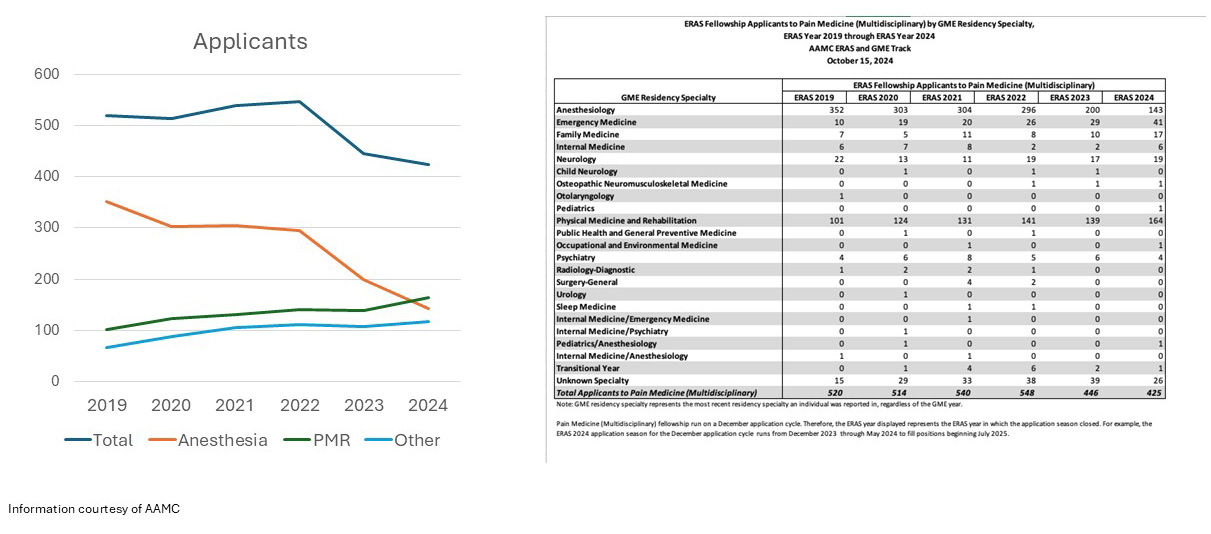
Figure 1: ERAS Fellowship Applicants to Pain Medicine by GME Residency Specialty - ERAS Year 2019 to 2024

With the foresight of this shifting landscape in pain medicine, ASRA Pain Medicine launched a PM&R working group in 2023 to enhance our resources and ensure we are meeting the needs of all individuals practicing in pain. This working group, led by Dr. Lynn Kohan, is providing personal outreach to PM&R members, new resources, and collaborative opportunities with all specialties in pain. This group recently released quality improvement (QI) templates for the American Board of Physical Medicine and Rehabilitation Maintenance of Certification Part IV. These templates offer members a guide and real-world examples for conducting quality improvement projects that satisfy these requirements. Guides currently available are for improving steroid safety and procedural practice and optimizing timeouts during pain management procedures. Thank you to Drs. Christine Hunt and Ameet Nagpal for this incredible asset for our members. Other members of the group (Drs. Alexios Carayannopoulos, Sayed Wahezi, Anishinder Parkash, Karson Mostert, Reed Yaras, and Bhavin Suther) are working on resources for practice management, neuromuscular ultrasound, and contract negotiations.
Areas for Future Growth
As mentioned earlier, we also received valuable and candid feedback from members who have not renewed. This insight expanded our understanding and reinforced our commitment to enhancing our offerings for members. Although many of us are excited about the atmosphere and educational environment of the annual meetings, only approximately 30% of members actually attend an in-person conference. Reasons for not attending include lack of time and travel support and loss of income from time out of the office and operating room. At ASRA Pain Medicine, we realize that we need to enhance and provide significant asynchronous learning methods for our members. We are currently investing in a state-of-the-art learning management system, and under the guidance of Dr. Stuart Grant, our CME Committee Chair, we will build a portfolio of educational opportunities for virtual learning. Additionally, Dr. Raj Gupta is assisting ASRA Pain Medicine in launching an improved monthly webinar series on clinically relevant topics, following an extensive information-gathering process. Individuals also discussed the need for education to maintain their certifications and licenses. In addition to the quality improvement templates mentioned earlier, we will also be creating these resources for the American Board of Anesthesiology Maintenance of Certification. Moreover, we paid close attention to when individuals said they needed practical content. At the fall meeting, we included billing and coding pearls at the end of each session for immediate use. We have also introduced ASRA Pain Medicine Connect, an online, members-only forum to start conversations, ask questions, and receive the clinically relevant information you need in real time. Additionally, we know that many pain management techniques suffer from low reimbursement, impacting access. With the advocacy tools discussed, we continue to push for proper reimbursement for scientifically proven pain control methods. Private practice members also make up a portion of ASRA Pain Medicine. It is also crucial that we understand their unique challenges and educational needs. The Private Practice SIG was one tool developed to enhance ASRA Pain Medicine’s offerings in this area. We appreciate the feedback from those who didn’t renew their membership and hope they will return to ASRA Pain Medicine once they see our new initiatives addressing their needs.
For a nonprofit to thrive, it needs a solid financial base. Using members’ money wisely is essential to support their clinical, research, and advocacy needs. Nonprofit doesn’t mean ignoring economic viability. To ensure ASRA Pain Medicine’s long-term success, the society must uphold its fiscal responsibility. Nonprofit hospitals need a 3%-6% operating margin to sustain community services. The board is dedicated to maintaining ASRA Pain Medicine’s strength. Lessons from other societies illustrate the problems that occur when fiduciary duties are neglected.
In summary, our members’ educational needs and preferences are constantly evolving. ASRA Pain Medicine will adapt and rise to the challenges within the fields of acute, transitional, and chronic pain management. We deeply appreciate our volunteers’ support, our members’ engagement, and our board’s exceptional leadership. Rest assured, ASRA Pain Medicine will celebrate its 100th anniversary. Meanwhile, we encourage you to attend the 50th Annual Regional Anesthesiology and Acute Pain Medicine Meeting in May 2025 as we celebrate the past, present, and future. Please reach out with any concerns or suggestions you believe we should address; we are here for you.