Global Warming and Ozone Depletion: The Real Cons of Nitrous Oxide Use
Cite as: Kelleher D, Fouts-Palmer EB. Global warming and ozone depletion: the real cons of nitrous oxide use. ASRA Pain Medicine News 2022;47. https://doi.org/10.52211/asra080122.032
The incorporation of nitrous oxide into anesthetic practice over 180 years ago introduced the possibility of pain-free surgery, allowing both the fields of surgery and anesthesiology to advance rapidly.1 With advances in pain management and the discovery of newer inhaled and IV anesthetics, the role of nitrous oxide in modern practice has been debated extensively. Over the past 30 years, these debates generally focus on whether the cardiopulmonary benefits of nitrous oxide outweigh the risk of postoperative nausea and vomiting (PONV) and toxicity to the patient and clinicians (Table 1).2-10 Despite a growing list of concerns, the reports almost always land in favor of continuing to use nitrous oxide (with appropriate PONV prophylaxis and scavenging) given the over 150 years of clinical evidence that it is “safe.”
Table 1: Summary of selected pro-con debates and reviews regarding use of nitrous oxide as an inhalational anesthetic from 1990 to today.
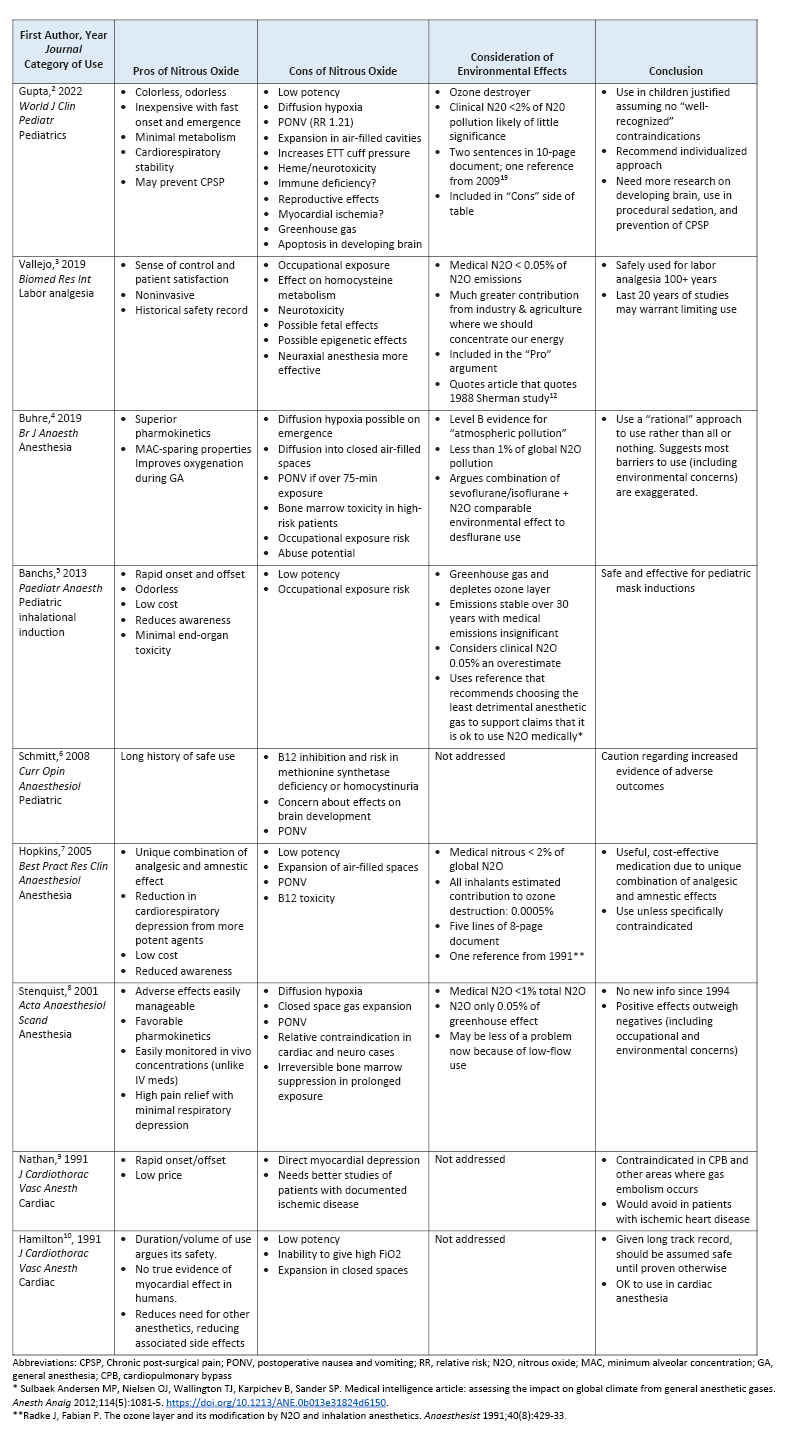
Unfortunately, these debates have acted as red herrings, distracting anesthesiologists from the true problem with nitrous oxide: its role as a potent greenhouse gas (GHG) and ozone destroyer. While concerns for nitrous oxide’s negative environmental effects were published as early as the 1970s, even recent pro-con debates fail to touch on this critical downfall.11 Potentially worse, when included, the effects are almost always dismissed as irrelevant, frequently citing the report that only a small percentage of nitrous oxide is from medical sources12 or postulating that it is no worse than desflurane (an odd pro argument given the global trend to severely restrict desflurane use for its detrimental environmental effects and the European Commission’s planned regulation to discourage the use of fluorinated GHGs with high global warming potential).4, 13 By not providing the relevant facts, including the global warming potential (GWP), ozone depleting potential (ODP), and lifetime in the atmosphere, the authors have further distracted anesthesiologists from understanding the true impact that nitrous oxide may have on climate change.
Nitrous oxide is debatably one of the most destructive anesthetic agents in use today.
Yet, nitrous oxide is debatably one of the most destructive anesthetic agents in use today.14 When compared with other inhaled agents, nitrous oxide has the longest lifetime in the atmosphere, exerting its effects on the environment for 114 years.15 In other words, the nitrous oxide used experimentally by anesthesiologists in Edinburgh in 1904 to perfect the art of nitrous-oxygen anesthesia remained in our atmosphere until 2018.16 Likewise, the nitrous oxide used to ease the labor pain of women today could outlive the children that they birth by 14 years or more. This is regardless of the use of waste anesthetic gas disposal (WAG-D) systems, as these systems are designed to limit exposure of the operating and labor room staff to anesthetic gasses, and, in most cases, are vented out into the atmosphere with no further processing.17 In fact, in many cases, the “WAG-D” line is ultimately connected to the same vacuum system as the “vacuum” line. The distinction is engineered to avoid loss of suction, not to avoid environmental pollution.17
The effect exerted for 114 years is not trivial. While nitrous oxide’s 20-year GWP (GWP20 289) is less than all other modern inhaled anesthetic agents (Table 2), it is almost 300 times greater than that of carbon dioxide and the only agent for which the GWP increases between 20 and 100 years.15 Additionally, the agent’s low potency requires much higher volumes to be effective, resulting in the cumulative effect of nitrous oxide use to be much more than sevoflurane when considered in clinically relevant volumes.19 When used as a carrier gas, nitrous oxide does not “save carbon” by reducing the fluorinated gas requirement, but, rather, exponentially worsens the 100-year carbon dioxide equivalent (CDE100) of an isoflurane or sevoflurane anesthetic.15 When considering all these facts, clinical nitrous oxide easily surpasses all other anesthetic agents, contributing greater than 99% of the total climate impact of anesthetic gases and 0.1% of all GHG emissions.20
Table 2: Properties of commonly used inhalational anesthetics with respect to environmental impact. Ozone depletion potential is calculated relative to CFC-11 (ODP=1). Global warming potential in carbon equivalents (GWP of CO2=1).

Nitrous oxide is also a potent ozone depleter, which further contributes to its impact on the environment. While the calculated ODP of nitrous oxide (0.017) may seem low (one half that of isoflurane), its stability over 100+ years allows the gas to reach the stratosphere in greater quantities.21 Additionally, when it reacts with the ozone, it creates a circular reaction that perpetuates its ozone-depleting effect: it breaks down to nitrogen dioxide, which subsequently reacts with oxygen to create more nitrous oxide.21 Its actual ODP also depends on the relative quantities of other elements in the atmosphere, with which it can undergo chemical reactions that result in other destructive compounds.22 Considering all anthropogenic sources (not just healthcare use), nitrous oxide is the largest and most impactful source of ozone depletion and expected to be throughout the 21st century.22 Ozone recovery is needed to prevent and reverse climate change, and nitrous oxide actively prevents this recovery.
As physicians, we should be maintaining the highest ethical standards and minimizing our impact on the health of our current and future patients.
Healthcare-related nitrous oxide use makes up only a small portion of total anthropogenic sources, contributing an estimated 0.05% of total GHG emissions compared with 5% for all anthropogenic nitrous oxide.12 Previous authors have indicated that healthcare’s contribution should be ignored and focus first should be placed on reducing nitrous oxide from agriculture and other industries. With the current “code red for humanity,” we argue that all industries should be made to reduce their anthropogenic nitrous oxide emissions, regardless of their relative contributions.23 As physicians, we should be maintaining the highest ethical standards and minimizing our impact on the health of our current and future patients.14 Reducing or eliminating nitrous oxide use at work is likely the biggest way an anesthesiologist can help slow climate change in any area of their life (other than eliminating desflurane use), equivalent to switching to a fully plant-based diet.24 Furthermore, as the healthcare industry is increasingly required to decarbonize just like any other industry, removing this potent GHG from use will be an easy and impactful first step in the road to reduced and net-zero emissions.14,25
Finally, we need to remain scientific in our recommendations and education of patients. We cannot continue to call on the “long history of nitrous oxide use” as a reason to continue its use. We now have many highly effective alternatives to nitrous oxide that do not have the same potential toxicity or long-lasting effects on the environment. Even if all the negative metabolic effects of nitrous oxide are proven clinically irrelevant, the agent’s known substantial contribution to climate change and the resultant adverse health effects on people around the world should prevent us from advertising its use as “safe.”26 At the very least, we need to inform our patients and the general public about this critical downside to nitrous oxide so that they may consider suitable alternatives for their pain control and anesthetic needs.

Deirdre C. Kelleher, MD, is an assistant professor of clinical anesthesiology at Weill Cornell Medicine in New York, NY.

E.B. Fouts-Palmer, MD, is an assistant professor of clinical anesthesiology at Weill Cornell Medicine in New York, NY.
References
- Pons PT. Nitrous oxide analgesia. Emerg Med Clin North Am 1988;6(4):777-82.
- Gupta N, Gupta A, Narayanan MRV. Current status of nitrous oxide use in pediatric patients. World J Clin Pediatr 2022;11(2):93-104. https://doi.org/10.5409/wjcp.v11.i2.93
- Vallejo MC, Zakowski MI. Pro-con debate: nitrous oxide for labor analgesia. Biomed Res Int 2019;2019:4618798. https://doi.org/10.1155/2019/4618798
- Buhre W, Disma N, Hendrickx J, et al. European Society of Anaesthesiology Task Force on Nitrous Oxide: a narrative review of its role in clinical practice. Br J Anaesth 2019;122(5):587-604. https://doi.org/10.1016/j.bja.2019.01.023
- Banchs R, Lerman J, Wald SH. The use of nitrous oxide as an adjuvant for inhalation inductions with sevoflurane: a pro-con debate. Paediatr Anaesth 2013;23(6):557-64. https://doi.org/10.1111/pan.12168
- Schmitt EL, Baum VC. Nitrous oxide in pediatric anesthesia: friend or foe? Curr Opin Anaesthesiol 2008;21(3):356-9. https://doi.org/10.1097/ACO.0b013e3282f8ad76
- Hopkins PM. Nitrous oxide: a unique drug of continuing importance for anaesthesia. Best Pract Res Clin Anaesthesiol 2005;19(3):381-9. https://doi.org/10.1016/j.bpa.2005.03.002
- Stenqvist O, Husum B, Dale O. Nitrous oxide: an ageing gentleman. Acta Anaesthesiol Scand 2001;45(2):135-7.
- Nathan HJ. Nitrous oxide is contraindicated in patients with coronary artery disease. Pro: nitrous oxide should not be used in patients with coronary artery disease. J Cardiothorac Vasc Anesth 1991;5(1):87-9. https://doi.org/10.1016/1053-0770(91)90101-x
- Hamilton WK. Nitrous oxide is contraindicated in patients with coronary artery disease. Con: nitrous oxide should be used in patients with coronary artery disease. J Cardiothorac Vasc Anesth 1991;5(1):90-1. https://doi.org/10.1016/1053-0770(91)90102-y
- Fox JW, Fox EJ, Villanueva R. Letter: Stratospheric ozone destruction and halogenated anaesthetics. Lancet 1975;1(7911):864. https://doi.org/10.1016/s0140-6736(75)93048-2
- Sherman SJ, Cullen BF. Nitrous oxide and the greenhouse effect. Anesthesiology 1988;68(5):816-7. https://doi.org/10.1097/00000542-198805000-00037
- Secretary-General of the European Commission. Proposal for a regulation of the European Parliament and of the Council on Fluorinated Greenhouse Gases, amending Directive (EU) 2019/1937 and repealing Regulation (EU) No 517/2014. Interinstitutional File: 2022/0099(COD). https://data.consilium.europa.eu/doc/document/ST-8042-2022-INIT/en/pdf. Published April 7, 2022. Accessed June 10, 2022.
- Beloeil H, Albaladejo P. Initiatives to broaden safety concerns in anaesthetic practice: the green operating room. Best Pract Res Clin Anaesthesiol 2021;35(1):83-91. https://doi.org/10.1016/j.bpa.2020.07.010
- Ryan SM, Nielsen CJ. Global warming potential of inhaled anesthetics: application to clinical use. Anesth Analg 2010;111(1):92-8. https://doi.org/10.1213/ANE.0b013e3181e058d7
- Daniell GW. On the administration of chloride of ethyl and somnoform, alone or in conjunction with nitrous oxide or ether. Br Med J 1904;1(2260):949-50. https://doi.org/10.1136/bmj.1.2260.949
- Welninski R. Which system should be used for waste anesthetic gas disposal. APSF Newsletter. 2014;29(1). https://www.apsf.org/article/which-system-should-be-used-for-waste-anesthetic-gas-disposal/ Accessed June 10, 2022.
- Lipana LS, Sherman J, Kanner O, et al. Yale Gassing Greener App. https://apps.apple.com/us/app/yale-gassing-greener/id1152700062 Last updated July 9, 2018. Accessed May 5,2022.
- McGain F. Why anaesthetists should no longer use nitrous oxide. Anaesth Intensive Care 2007;35(5):808-9.
- Gadani H, Vyas A. Anesthetic gases and global warming: potentials, prevention and future of anesthesia. Anesth Essays Res 2011;5(1):5-10. https://doi.org/10.4103/0259-1162.84171
- Lopes R, Shelton C, Charlesworth M. Inhalational anaesthetics, ozone depletion, and greenhouse warming: the basics and status of our efforts in environmental mitigation. Curr Opin Anaesthesiol 2021;34(4):415-20. https://doi.org/10.1097/ACO.0000000000001009
- Ravishankara AR, Daniel JS, Portmann RW. Nitrous oxide (N2O): the dominant ozone-depleting substance emitted in the 21st century. Science 2009;326(5949):123-5. https://doi.org/10.1126/science.1176985
- United Nations. Secretary-general calls latest IPCC climate report ‘code red for humanity’, stressing ‘irrefutable’ evidence of human influence. https://www.un.org/press/en/2021/sgsm20847.doc.htm#:~:text=Today's%20IPCC%20Working%20Group%201,of%20people%20at%20immediate%20risk Published August 9, 2021. Accessed May 5,2022.
- Eisen MB, Brown PO. Rapid global phaseout of animal agriculture has the potential to stabilize greenhouse gas levels for 30 years and offset 68 percent of CO2 emissions this century. PLOS Clim;2022:1(2). https://doi.org/10.1371/journal.pclm.0000010
- Dzau VJ, Levine R, Barrett G, et al. Decarbonizing the U.S. health sector - a call to action. N Engl J Med 2021;385(23):2117-9. https://doi.org/10.1056/NEJMp2115675
- Xu R, Yu P, Abramson MJ, et al. Wildfires, global climate change, and human health. N Engl J Med 2020;383(22):2173-81. https://doi.org/10.1056/NEJMsr2028985