POCUS Spotlight: Peripherally Inserted Central Catheter (PICC) Insertion
Cite as: Mehra C, Dhar P. POCUS spotlight: peripherally inserted central catheter (PICC) insertion. ASRA Pain Medicine News 2026;51. https://doi.org/10.52211/asra050126.009.
POCUS Spotlight
Introduction
The ability to obtain venous access is one of the most fundamental yet crucial components for a large number of diagnostic and therapeutic interventions.1-4 Peripherally inserted central catheters (PICCs) are a subset of central venous catheters. They are 50 cm to 60 cm long single, double, or triple lumen catheters that are placed in a peripheral arm vein and terminate in the intrathoracic venous system. A properly placed PICC may facilitate a transition from a medical care facility to home for intermittent intravenous therapy.5 The failure rate of PICCs continues to be as high as 40%, leading to interruption of therapy.6-10
Indications
PICCs are indicated in patients who require venous access for several weeks.11 Common indications include patients with limited peripheral venous access, long-term intravenous medication administration, including total parenteral nutrition and blood product infusions, and frequent blood sampling.
Contraindications
Relative contraindications for PICCs include burns, trauma, skin infections, a history of venous thrombosis at the insertion site, active bacteremia, the presence of a hemodialysis fistula on the ipsilateral limb, small diameter of arm veins (smaller than 3 mm to 4 mm), and complete axillary lymph node dissection.12
Relevant Venous Anatomy
PICCs are placed through the basilic, brachial, cephalic, or medial cubital vein of the arm.13
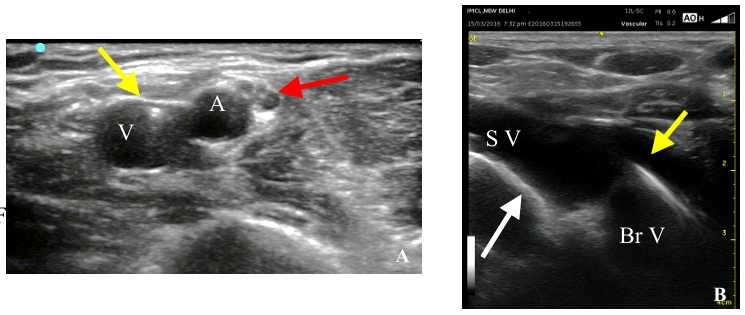
The upper limb is drained by superficial and deep venous systems. The superficial venous system includes the cephalic, basilic, median cubital, and median antebrachial veins. The subclavian and axillary veins form the proximal group, while the brachial, radial, and ulnar veins form the distal group of the venous system. (Figure 1)
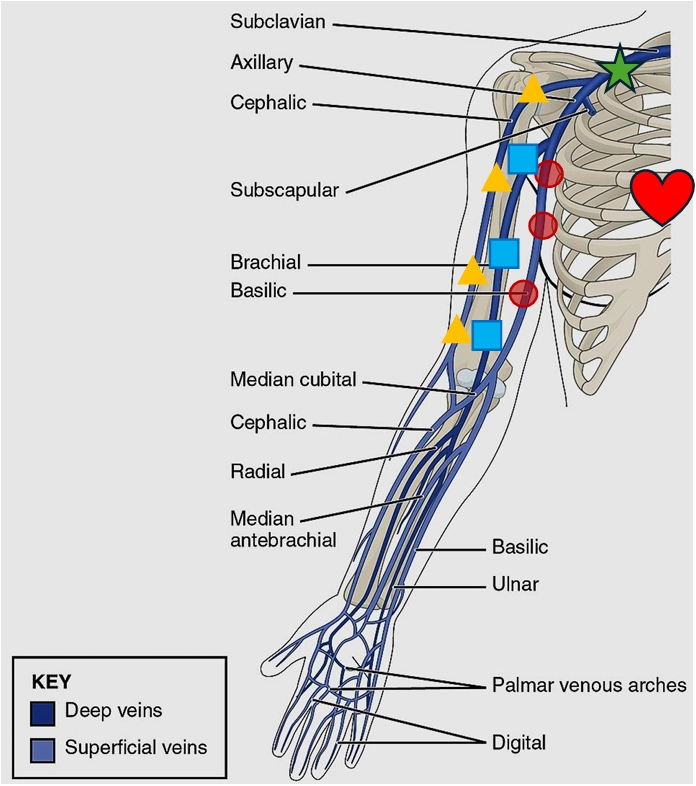
The basilic vein is preferred because of its superficial location and larger size. It has a comparatively straighter route to the superior vena cava (SVC) and provides a shallower angle for needle insertion.
The cephalic vein is smaller than the basilic vein. It offers a sharp-angle needle insertion and a tortuous course and carries a higher incidence of mechanical phlebitis.
The brachial vein is larger in size, runs a shorter course, and is located deeper than the basilic vein. There is a higher risk of inadvertent neurovascular injury because it runs alongside the brachial artery and the median nerve.
The median cubital vein joins the basilic vein and is prominent in the antecubital fossa. It carries a higher risk of mechanical phlebitis, owing to constant bending at the elbow crease.
Equipment
PICCs vary in length (50 cm to 60 cm), size (3, 4, or 5 French (Fr)), and the number of lumens (single to triple). Standard equipment while using the modified Seldinger technique includes:4,14,15
- High-frequency linear ultrasound transducer with sterile probe sheath cover
- Sterile drapes
- Tape measure
- Heparinized saline flush
- PICC insertion kit contents (Figure 2): PIC catheter, introducer needle, soft-tip guidewire, skin track dilator, catheter fixation device, and needle-free connector device

Appropriate Insertion Technique for PICC
PICC insertion involves a sequential approach that encompasses evaluation of a suitable vein, its cannulation, and confirmation of a safe PICC tip location.16
Pre-procedural evaluation and target vein selection
The venous anatomy is assessed at the antecubital fossa, bicipital-humeral groove, axilla, and the supraclavicular and infraclavicular fossae, as shown in Figures 1 and 3 and Video 1. Veins are selected in order of preference, starting with the basilic vein in the bicipital-humeral groove, followed by the brachial veins within the neurovascular bundle of the arm, and then the axillary vein. A stepwise approach is recommended for selecting a suitable vein using the rapid peripheral vein assessment (RaPeVA) protocol, as outlined in Table 1.17-23

| Step | Clinical Reference |
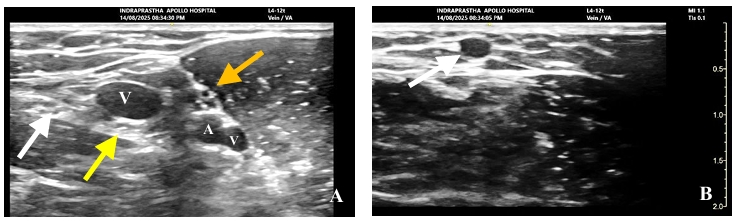
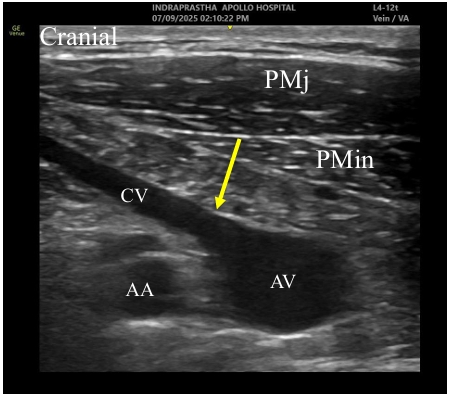
| Identify the median nerve and brachial artery prior to venipuncture.(Figure 4) | A trans-neural puncture in a sedated patient or an arterial puncture in a patient with a deranged coagulation profile can lead to nerve damage or an expanding hematoma, respectively.22,24 |
| Measure the diameter and depth of the selected vein. | Vessels within 0.3-1.5 cm of the surface and greater than 4 mm in diameter have a higher cannulation rate and longer PICC endurance.25-27(Figure 4 and Video 2) |
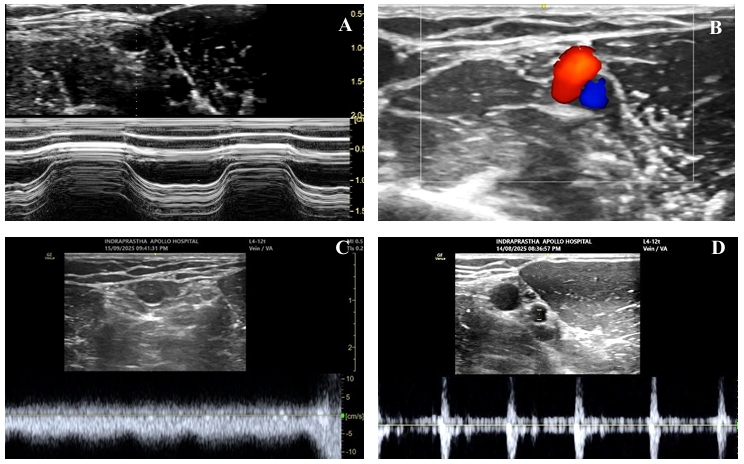
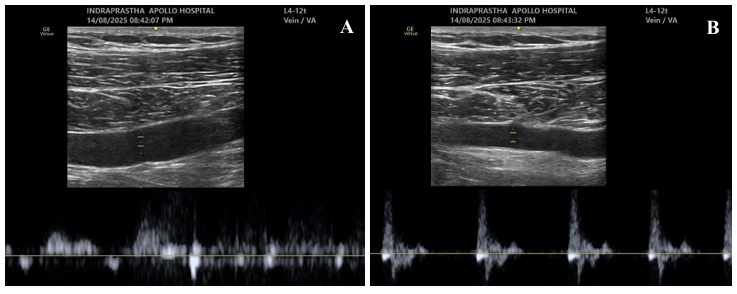
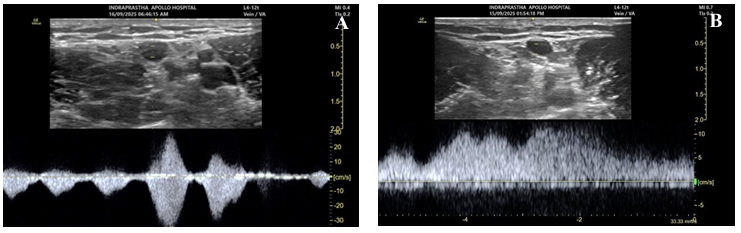
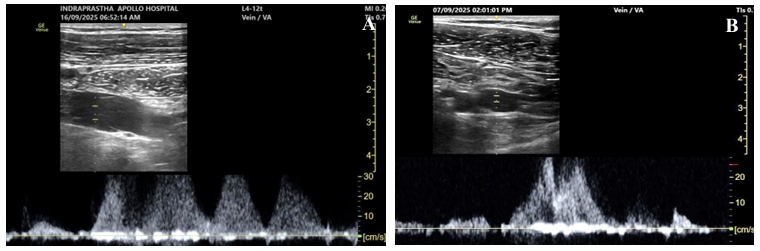
| Evaluate the vessels for patency.28-37 | 1. Sequential compression using B-mode and/or M-mode ultrasound. (Figure 5 and Video 3) 2. Phasic variation in blood flow with respiration and arterial pulsations with color flow doppler or pulse wave doppler (PWD) modes. (Figures 5 and 6) 3. Augmentation of blood flow with fore-arm compression or tight hand grip using color doppler or PWD. (Figures 7 and 8 and Video 4) 4. Augmentation of blood flow with deep inspiration using color flow doppler or PWD. (Figure 7 and Video 5) |
| Identify the location of valves and exclude the possibility of thrombus or external compression by any mass.38 (Video 6) |
Choice of PICC size
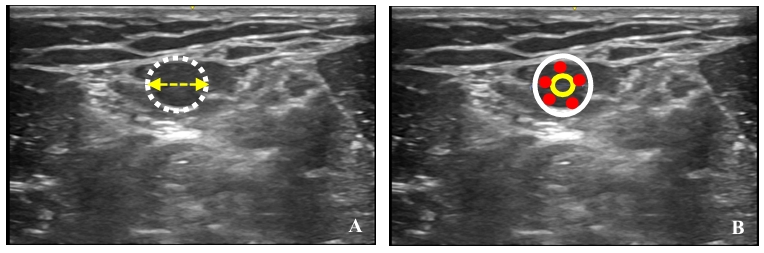
Estimate the transverse diameter (or circumference of the vein) by applying minimum transducer compression. The ideal catheter-vein ratio is ≤ 1:3 (This leaves at least two-thirds of the vein diameter free for the flow surrounding the catheter.)39 A cut-off point of 45% has been found to predict thrombosis.24,40-43 (Figure 9). A 1 Fr catheter size corresponds to 0.33 mm. This implies that a 3 Fr catheter requires a vein diameter of at least 3 mm. Presumably, a larger PICC size can obstruct blood flow from superficial to deep veins via the perforators, leading to obstructed or sluggish flow. (Video 7)
Cutaneous Exit-site Location
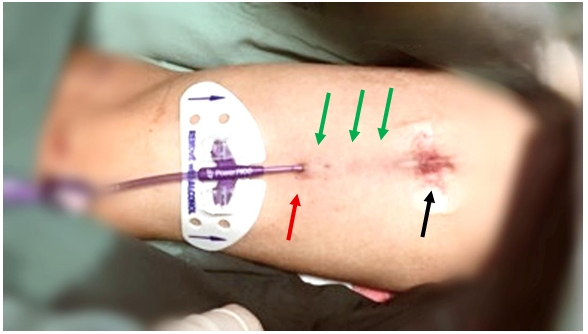
Once an appropriate vein has been selected, the clinician should judiciously plan the exit site for the catheter (before proceeding with venipuncture). This involves division of the upper arm into three segments, which is the zone insertion method™ (ZIM).44 (Figure 10 and Table 2)
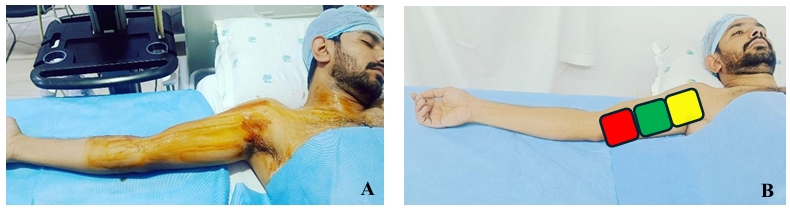
| ZONES | CLINICAL RELEVANCE |
| Yellow zone (proximal third of the arm) | This has a higher degree of bacterial contamination of the skin due to the proximity of the axilla.18 |
| Green zone (middle third of the arm) | This is considered the ideal site for venipuncture. |
| Red zone (distal third of the arm) | This carries a higher risk of PICC dislodgment because of elbow movements. Hence, the red zone should be avoided at both the venipuncture site and the catheter exit site. |
Appropriate Aseptic Technique
PICC insertion requires adopting maximal barrier precautions. The use of a sterile cover for the transducer and the cable, especially when resting on the sterile field, is recommended.22,23,45,46
Ultrasound-guided venipuncture
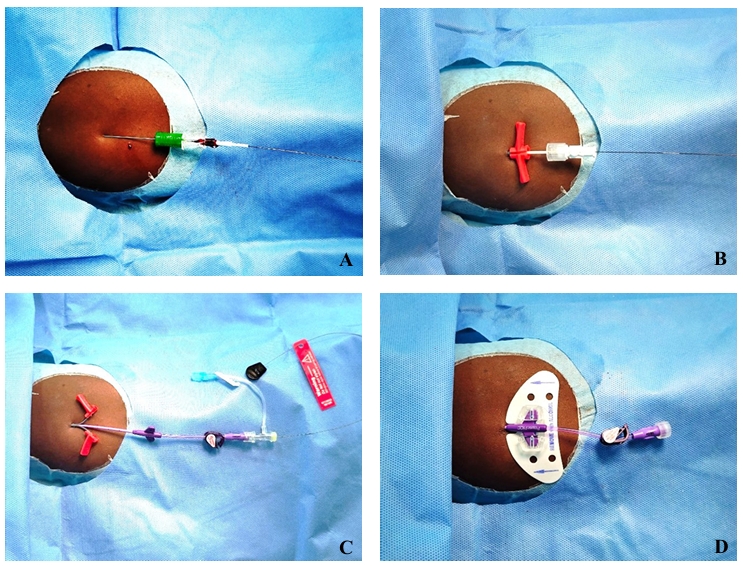
Ultrasound-guided venipuncture can be performed by visualizing the target vein in its short, long, or oblique axis, using either in-plane or out-of-plane needle insertion.23,47-50 The modified Seldinger technique should be preferentially used for venipuncture.51-54 (Figures 11, 12, and Video 8) Adjust the operating table, patient’s arm, and the ultrasound machine to best suit the ergonomics.
Navigation of PICC Guidewire Through the Vessel and Confirmation of an Acceptable Guidewire Tip Location Using Ultrasound
The guidewire advancement should be tracked along its course, starting from the venipuncture site and across the vessels in the supra/ infraclavicular fossae. The guidewire and catheter tip location should also be confirmed at the cavo-atrial junction prior to the conclusion of the PICC placement procedure. The ECHOTIP protocol provides valuable input for guidewire tracking when ultrasound is used as a navigational tool.17,18,20,55-58
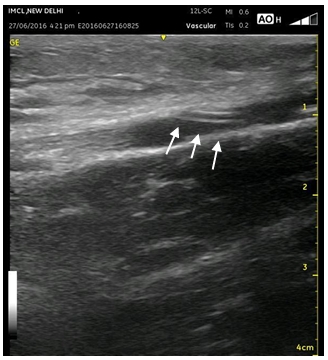
Ultrasound-assisted intraprocedural guidewire-tip navigation: Ultrasound tracks the guidewire course through the axillary, subclavian, and brachiocephalic veins to its termination in the SVC.22,59 A 7-12 MHz linear transducer is used to visualize the guidewire inside the lumen of the cannulated vein and up to the axillary and subclavian veins in the infra or supraclavicular fossae. (Figures 12, 13 and Video 9) A linear transducer placed over the supraclavicular fossa helps to trace the guidewire within the subclavian and brachiocephalic trunk.60,61 The ultrasound appearance of the guidewire transit from the subclavian vein to the brachiocephalic trunk gives the appearance of “sparkling guidewire” and has been termed as “sparkling guidewire sign” by the authors. (Figure 12 and Video 10)
Ultrasound-assisted intraprocedural guidewire-tip localization: The use of various intraprocedural methods for catheter tip localization at the cavo-atrial junction is recommended by current guidelines.22,23,58,62-64 A phased array echo probe is used for confirming tip location using apical four-chamber or subcostal views.
Direct method: It involves direct visualization of the tip of the catheter at the junction between the SVC and right atrium (RA) or between the RA and the IVC (for PICC inserted through the femoral route). In practical usage, the catheter tip is initially visualized within the RA cavity and withdrawn slightly to rest at the SVC-RA junction.60,61,65-70
Indirect method: “Bubble test” is the rapid injection of 5-10 ml of agitated normal saline through the catheter. The appearance of a cloud of microbubbles in the RA in less than 2 seconds confirms the tip placement in the proximity of RA.52,71-78 (Video 11) A delay in the appearance of microbubbles of more than 2 seconds correlates with an incorrect tip placement.70 As the PICCs are longer and narrower than a proximally inserted central venous catheter (CVC), a cut-off limit of 2 seconds is higher than that suggested for CVC (1 second).79
Other methods for intra-procedural tip confirmation include intracavitary electrocardiogram, fluoroscopy and the use of pre-insertion anthropometric algorithms.22,23,80-82 Post-procedure catheter manipulation is not supported by current guidelines.22,23,83
Measures to Secure PICC Exit-site:
A secure dressing and catheter stabilization approach helps minimize micro-motion and reduces the risk of vein thrombosis and PICC fracture.22,23,45,46,84,85 Strategies for protecting the exit site include subcutaneous tunneling of the proximal portion of the catheter, using cyanoacrylate adhesive to seal both the catheter exit and venipuncture sites,86-90 and catheter design modifications, such as a reverse-tapered diameter to prevent backflow of infused fluid.91
Rationale for Tunneling
Subcutaneous tunneling of a PIC catheter allows for relocation of the exit site away from the skin puncture site. This is especially helpful in patients with complex vascular access, cognitive dysfunction, and a need for long-term parenteral nutrition.92-100 (Figure 14) For example, for a PICC inserted in the yellow zone, an exit site can be chosen in the green zone by tunneling the bare portion of the catheter (Rapid Assessment of Vascular Exit Site and Tunneling Options [RAVESTO] Protocol).23,101 Tunneling can be performed using a dedicated tunneling device or a peripheral intravenous cannula.92-100,102,103
PICC Fixation and Dressing Specifications
Cover the exit site with a semi-permeable, transparent membrane dressing, preferably with a moisture vapor transfer rate of 1,500 g/m2/day or more.6,104 Fixation may be done with a sutureless, securement device that secures winged catheters, such as PICCs.12,105-109 (Figure 11). The extra portion of PICC staying outside the exit site should be curled back to protect the catheter from being accidentally pulled or kinked at the elbow crease. This portion should be covered by a separate dressing or device.
Ultrasound Guidance to Avoid Malposition of PICC
Malposition of a PICC involves unintentional placement into the ipsilateral internal jugular vein or the contralateral subclavian vein or curling back within the ipsilateral subclavian vein and tracking toward the axillary vein, where it may coil in the axilla.65 Reported rates of PICC malposition range from 35%-65%.110
Malposition can be avoided by carefully following the guidewire and catheter passage through the veins using sonographic guidance as described earlier.
Safe use of PICCs (Instructions for Caregivers and End Users)
The risk of infection increases with every interruption to the closed system.111,112 A “closed system” should be maintained at the open end of the catheter by the use of a sterile, self-sealing, swabable, needle-free access connector.6,111 Use “push-pause technique” or “positive pressure finish” to flush and lock the catheters. Flush and lock the catheter with heparinized saline (10 units/ml) after each use. (Video 12) The use of smaller-volume syringes to flush a blocked catheter can generate higher internal pressure and increase the risk of catheter rupture.113 A total break can result in possible catheter embolus.
Overview of the Technique of PICC Insertion
The following are the steps for the sterile, modified Seldinger technique:
- Informed and written consent from the patient.
- Make a note of the patient’s ipsilateral arm circumference at 10 cm from the elbow crease. This can help the clinician to compare arm swelling later as a possible complication of PICC.
- Adjust the operating table, patient’s arm. and the ultrasound machine to best suit the ergonomics.
- Conduct pre-procedure ultrasound scan for assessment of a suitable vein for cannulation (RaPeVa Protocol).
- Assess the vein-to-catheter ratio for the desired catheter size.
- Mark the course of the chosen vein with a skin marking pen. This helps to track the guidewire and catheter from the insertion point to the ipsilateral subclavian vein.
- Expose, clean, and drape the ipsilateral arm, supra-clavicular and infra-clavicular regions, neck, and suprasternal notch. This helps to scan these regions for guidewire navigation without compromising the sterility of the ultrasound transducer during PICC insertion.
- Use maximum barrier precautions during the insertion procedure.
- Use the Dawson’s ZIMTM protocol to select the venipuncture and exit site.
- Raise the skin weal with local anesthetic.
- In a step-wise manner, access the vein with a venipuncture needle and thread the guidewire through the puncture needle.
- Use the ECHOTIP protocol for intraprocedural navigation of guidewire and the final tip location at SVC-RA junction.
- Dilate the skin track using the dilator and peel-away introducer set. Peel and remove the peel away introducer while keeping the dilator in place. Railroad the catheter over the guidewire, or remove the guidewire and introduce the styletted catheter per the manufacturer’s instructions.
- Use the RAVESTO protocol for assessment of PICC exit-site and securement strategies.
- Flush the catheter with heparinized saline solution.
Complications Related to PICC
Factors potentiating the risk of complications include arterial or nerve injury, suboptimal catheter tip location, exit site in red or yellow zone, along with poor fixation methods, and lack of asepsis.4,16,22,23,40,45,46,64,114-12
Commonly encountered complications include thrombophlebitis and catheter dislodgement, defined as a change in the catheter’s position of more than 2 cm from its original location without affecting function. This can potentially lead to vessel wall perforation and extravasation.4,6 Other complications include catheter-related infection,11,124-133 catheter-related thrombosis, and catheter blockage.134
Additional Useful Tips
A single useful tip for the assessment of patency of both the superficial and deep venous system simultaneously, using the principles described previously, has been named by the authors as “axillo-cephalic-deep inspiration-valsalva assessment technique (ACIVA technique).” A linear ultrasound transducer is placed in the supraclavicular fossa, and the drainage of the cephalic vein into the axillary and subclavian veins is assessed. These veins collapse completely with the coaptation of their anterior and posterior walls with deep inspiration and expand with the Valsalva maneuver. (Video 13)
Importance of examining cephalic vein confluence with the axillary vein:
This confluence is an area of increased turbulence. Often, a valve is found in the cephalic vein just prior to its junction with the axillary vein. Gentle cranio-caudal tilt of the linear ultrasound transducer, while visualizing the distal subclavian vein at both supra and infraclavicular regions, aligns the cephalic vein with the subclavian vein. (Figure 15 and Video 14)
“Peripheral Venous Swirl Test”: In patients with challenging venous access, eg, contractures over the shoulder or elbow, the clinician can flush 5 ml of agitated saline through the IV cannula or the venipuncture needle (proximal to the elbow) and observe the swirl within the subclavian or brachiocephalic trunk (termed as Peripheral Venous Swirl Test by the authors). This is followed by PICC insertion, using the modified Seldinger technique.135 (Video 15)
Conclusion
The use of strategies outlined in this article allows the clinician to confidently use ultrasound for preliminary venous assessment, real-time venipuncture, guidewire tip navigation, and guidewire and catheter tip location, as well as for the evaluation of some late non-infective complications.
Further, the use of needle-free injectable ports, sutureless securement techniques, maximum barrier precautions, the appropriate choice of exit site, and tunneling the distal portion of the PICC increases the safety profile and the cost-effectiveness of the procedure.4,25,31,32,50,62,63,73,125-132


References
- Arul GS, Livingstone H, Bromley P, et al. Ultrasound-guided percutaneous insertion of 2.7 Fr tunneled Broviac lines in neonates and small infants. Pediatr Surg Int 2010;26(8):815-8. https://doi.org/10.1007/s00383-010-2616-3
- Akers AS, Chelluri L. Peripherally inserted central catheter use in the hospitalized patient: is there a role for the hospitalist? J Hosp Med 2009;4(6): E1-4. https://doi.org/10.1002/jhm.446
- Yamada R, Morita T, Yashiro E, et al. Patient-reported usefulness of peripherally inserted central venous catheters in terminally ill cancer patients. J Pain Symptom Manage2010;40(1):60-6. https://doi.org/10.1016/j.jpainsymman.2009.11.327
- Gao Y, Liu Y, Ma X, et al. The incidence and risk factors of peripherally inserted central catheter-related infection among cancer patients. Ther Clin Risk Manag 2015;11:863-71. https://doi.org/10.2147/TCRM.S83776
- Fields JM, Piela NE, Au AK, et al. Risk factors associated with difficult venous access in adult ED patients. Am J Emerg Med 2014;32(10):1179-82. https://doi.org/10.1016/j.ajem.2014.07.008
- Jacobson AF, Winslow EH. Variables influencing intravenous catheter insertion difficulty and failure: an analysis of 339 intravenous catheter insertions. Heart Lung 2005;34(5):345-59. https://doi.org/10.1016/j.hrtlng.2005.04.002
- Chopra V, Ratz D, Kuhn L, et al. PICC-associated bloodstream infections: prevalence, patterns, and predictors. Am J Med 2014;127(4):319-28. doi: https://doi.org/10.1016/j.amjmed.2014.01.001
- Chan RJ, Northfield S, Larsen E, et al. Central venous access device securement and dressing effectiveness for peripherally inserted central catheters in adult acute hospital patients (CASCADE): a pilot randomised controlled trial. Trials 2017;18(1):458. https://doi.org/10.1186/s13063-017-2207-x
- Yap YS, Karapetis C, Lerose S, et al. Reducing the risk of peripherally inserted central catheter line complications in the oncology setting. Eur J Cancer Care (Engl) 2006;15(4):342-7. https://doi.org/10.1111/j.1365-2354.2006.00664.x
- Yamamoto AJ, Solomon JA, Soulen MC, et al. Sutureless securement device reduces complications of peripherally inserted central venous catheters. J Vasc Interv Radiol2002;13(1):77-81. https://doi.org/10.1016/s1051-0443(07)60012-8
- Bolz K, Ramritu P, Halton K, et al. Management of central venous catheters in adult intensive care units in Australia: policies and practices. Healthc Infect 2008;13(2):48-55. https://doi.org/10.1071/HI08016
- Ullman AJ, Marsh N, Mihala G, et al. Complications of central venous access devices: a systematic review. Pediatrics 2015;136(5):e1331-44. https://doi.org/10.1542/peds.2015-1507
- O’Grady NP, Alexander M, Burns LA, et al Healthcare Infection Control Practices Advisory Committee. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control 2011;39(4 Suppl 1):S1-34. https://doi.org/10.1016/j.ajic.2011.01.003
- Smith B, Royer TI. New standards for improving peripheral i.v. catheter securement. Nursing 2007;37(3):72-4. : https://doi.org/10.1097/01.nurse.0000261859.31596.3e
- Gonzalez R, Cassaro S. Percutaneous central catheter (archived). 2023 Sep 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–.
- Meyer P, Cronier P, Rousseau H, et al. Difficult peripheral venous access: clinical evaluation of a catheter inserted with the Seldinger method under ultrasound guidance. J Crit Care2014;29(5):823-7. https://doi.org/10.1016/j.jcrc.2014.04.022
- Ash AJ, Raio C. Seldinger technique for placement of “peripheral” internal jugular line: novel approach for emergent vascular access. West J Emerg Med 2016;17(1):81-3. https://doi.org/10.5811/westjem.2015.11.28726
- .Duran-Gehring P, Bryant L, Reynolds JA, et al. Ultrasound-guided peripheral intravenous catheter training results in physician-level success for emergency department technicians. J Ultrasound Med 2016;35(11):2343-52. https://doi.org/10.7863/ultra.15.11059
- Witting MD, Schenkel SM, Lawner BJ, et al. Effects of vein width and depth on ultrasound-guided peripheral intravenous success rates. J Emerg Med 2010;39(1):70-5. https://doi.org/10.1016/j.jemermed.2009.01.003
- White A, Lopez F, Stone P. Developing and sustaining an ultrasound-guided peripheral intravenous access program for emergency nurses. Adv Emerg Nurs J 2010;32:173-88. https://doi.org/10.1097/TME.0b013e3181dbca70
- Miles G, Salcedo A, Spear D. Implementation of a successful registered nurse peripheral ultrasound-guided intravenous catheter program in an emergency department. J Emerg Nurs2012;38(4):353-6. https://doi.org/10.1016/j.jen.2011.02.011
- Laksonen RP Jr, Gasiewicz NK. Implementing a program for ultrasound-guided peripheral venous access: training, policy and procedure development, protocol use, competency, and skill tracking. Nurs Clin North Am 2015;50(4):771-85. https://doi.org/10.1016/j.cnur.2015.07.010
- .American College of Emergency Physicians. Emergency ultrasound guidelines. Ann Emerg Med 2009;53(4):550-70. https://doi.org/10.1016/j.annemergmed.2008.12.013
- Brescia F, Pittiruti M, Spencer TR, et. The SIP protocol update: eight strategies, incorporating rapid peripheral vein assessment (RaPeVA), to minimize complications associated with peripherally inserted central catheter insertion. J Vasc Access 2024;25(1):5-13.https://doi.org/10.1177/11297298221099838.
- Emoli A, S, Marche B, et al. The ISP (safe insertion of PICCs) protocol: a bundle of 8 recommendations to minimize the complications related to the peripherally inserted central venous catheters (PICC). Assist Inferm Ric 2014;33(2):82-9. Italian. https://doi.org/10.1702/1539.16813
- Brescia F, Pittiruti M, Ostroff M, et al. The SIC protocol: a seven-step strategy to minimize complications potentially related to the insertion of centrally inserted central catheters. J Vasc Access 2023;24(2):185-190. https://doi.org/10.1177/11297298211036002
- Brescia F, Pittiruti M, Ostroff M, et al. The SIF protocol: a seven-step strategy to minimize complications potentially related to the insertion of femorally inserted central catheters. J Vasc Access 2023;24(4):527-34. https://doi.org/10.1177/11297298211041442
- Spencer TR, Pittiruti M. Rapid central vein assessment (RaCeVA): a systematic, standardized approach for ultrasound assessment before central venous catheterization. J Vasc Access2019;20(3):239-49. https://doi.org/10.1177/1129729818804718
- Brescia F, Pittiruti M, Ostroff M, et al. Rapid femoral vein assessment (RaFeVA): a systematic protocol for ultrasound evaluation of the veins of the lower limb, so to optimize the insertion of femorally inserted central catheters. J Vasc Access 2021;22(6):863-72. https://doi.org/10.1177/1129729820965063
- Dawson RB. PICC Zone Insertion Method™ (ZIM™): a systematic approach to determine the ideal insertion site for PICCs in the upper arm. J Assoc Vasc Access 2011;16(3): 156–65. https://doi.org/10.2309/java.16-3-5
- Gorski LA, Hadaway L, Hagle ME, et al. Infusion therapy standards of practice, 8th Edition. J Infus Nurs 2021;44(1S Suppl 1):S1-S224. https://doi.org/10.1097/NAN.0000000000000396.Lamperti M, Biasucci DG, Disma N, et al European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol 2020;37(5):344-76.https://doi.org/10.1097/EJA.0000000000001180 Erratum in: Eur J Anaesthesiol2020;37(7):623. https://doi.org/10.1097/EJA.0000000000001257
- Pittiruti M, Scoppettuolo G. Raccomandazioni GAVeCeLT 2021 per l’indicazione, l’impianto e la gestione dei dispositivi per accesso venoso, 2021, https://gavecelt.it/nuovo/sites/default/files/uploads/Raccomandazioni%20GAVeCeLT%202021.pdf
- Panebianco NL, Fredette JM, Szyld D, et al. What you see (sonographically) is what you get: vein and patient characteristics associated with successful ultrasound-guided peripheral intravenous placement in patients with difficult access. Acad Emerg Med 2009;16(12):1298-1303. https://doi.org/10.1111/j.1553-2712.2009.00520.x
- Fields JM, Dean AJ, Todman RW, et al. The effect of vessel depth, diameter, and location on ultrasound-guided peripheral intravenous catheter longevity. Am J Emerg Med2012;30(7):1134-40. https://doi.org/10.1016/j.ajem.2011.07.027
- Nasra K, Negussie E. Sonography vascular peripheral vein assessment, protocols, and interpretation. 2023 Feb 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–.
- Baker M, Anjum F, dela Cruz J. Deep venous thrombosis ultrasound evaluation. 2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–.
- Pomero F, Dentali F, Borretta V, et al. Accuracy of emergency physician-performed ultrasonography in the diagnosis of deep-vein thrombosis: a systematic review and meta-analysis. Thromb Haemost 2013;109(1):137-45. https://doi.org/10.1160/TH12-07-0473
- Rose SC, Nelson TR. Ultrasonographic modalities to assess vascular anatomy and disease. J Vasc Interv Radiol 2004;15(1 Pt 1):25-38. https://doi.org/10.1097/01.rvi.0000106395.63463.59
- Weber TM, Lockhart ME, Robbin ML. Upper extremity venous Doppler ultrasound. Radiol Clin North Am 2007;45(3):513-24. https://doi.org/10.1016/j.rcl.2007.04.005
- Chin EE, Zimmerman PT, Grant EG. Sonographic evaluation of upper extremity deep venous thrombosis. J Ultrasound Med 2005;24(6):829-38; quiz 839-40. https://doi.org/10.7863/jum.2005.24.6.829
- Baarslag HJ, van Beek EJ, Koopman MM, et al. Prospective study of color duplex ultrasonography compared with contrast venography in patients suspected of having deep venous thrombosis of the upper extremities. Ann Intern Med 2002;136(12):865-72. https://doi.org/10.7326/0003-4819-136-12-200206180-00007. Erratum in: Ann Intern Med2003;138(5):438.
- Tan G, Ng M. Emergency department point-of-care ultrasound for upper extremity deep venous thrombosis ED POCUS for upper extremity DVT. Int J Emerg Med 2021;14(1):66. https://doi.org/10.1186/s12245-021-00391-4
- Moore C. An emergency department nurse-driven ultrasound-guided peripheral intravenous line program. J Assoc Vasc Access 2013;18:45. https://doi.org/10.1016/j.java.2012.12.001
- Sosthène TV, Serge KK, Medard KK, et al. Duplex ultrasound in upper and lower limb deep venous thrombosis. Ann Circ 2020;5(1): 001-7. https://doi.org/10.17352/ac.000015
- Grant JD, Stevens SM, Woller SC, et al. Diagnosis and management of upper extremity deep-vein thrombosis in adults. Thromb Haemost 2012;108(6):1097-108. https://doi.org/10.1160/TH12-05-0352
- Loveday HP, Wilson JA, Pratt RJ, et al. UK Department of Health. epic3: national evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2014;86 Suppl 1:S1-70. https://doi.org/10.1016/S0195-6701(13)60012-2
- O’Grady NP, Alexander M, Burns LA, et al. Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 2011;52(9):e162-93. https://doi.org/10.1093/cid/cir257
- Pinelli F, Pittiruti M, Annetta MG, et al. A GAVeCeLT consensus on the indication, insertion, and management of central venous access devices in the critically ill. J Vasc Access2025;26(4):1096-1114. https://doi.org/10.1177/11297298241262932
- Spencer TR, Mahoney KJ. Reducing catheter-related thrombosis using a risk reduction tool centered on catheter to vessel ratio. J Thromb Thrombolysis 2017;44(4):427-34. https://doi.org/10.1007/s11239-017-1569-y
- Sharp R, Cummings M, Fielder A, et al. The catheter to vein ratio and rates of symptomatic venous thromboembolism in patients with a peripherally inserted central catheter (PICC): a prospective cohort study. Int J Nurs Stud 2015;52(3):677-85. https://doi.org/10.1016/j.ijnurstu.2014.12.002
- Sharp R, Carr P, Childs J, et al. Catheter to vein ratio and risk of peripherally inserted central catheter (PICC)-associated thrombosis according to diagnostic group: a retrospective cohort study. BMJ Open 2021;11(7):e045895. https://doi.org/10.1136/bmjopen-2020-045895
- Nifong TP, McDevitt TJ. The effect of catheter to vein ratio on blood flow rates in a simulated model of peripherally inserted central venous catheters. Chest 2011;140(1):48-53. https://doi.org/10.1378/chest.10-2637
- Biasucci DG, La Greca A, Scoppettuolo G, et al. Ultrasound-guided central venous catheterization: it is high time to use a correct terminology. Crit Care Med 2015;43(9):e394-6.https://doi.org/10.1097/CCM.0000000000001069
- Phelan M, Hagerty D. The oblique view: an alternative approach for ultrasound-guided central line placement. J Emerg Med 2009;37(4):403-8. https://doi.org/10.1016/j.jemermed.2008.02.061
- Dilisio R, Mittnacht AJ. The “medial-oblique” approach to ultrasound-guided central venous cannulation–maximize the view, minimize the risk. J Cardiothorac Vasc Anesth2012;26(6):982-4. https://doi.org/10.1053/j.jvca.2012.04.013
- Wilson JG, Berona KM, Stein JC, et al. Oblique-axis vs. short-axis view in ultrasound-guided central venous catheterization. J Emerg Med 2014;47(1):45-50. https://doi.org/10.1016/j.jemermed.2013.11.080
- Egan G, Healy D, O’Neill H, et al. Ultrasound guidance for difficult peripheral venous access: systematic review and meta-analysis. Emerg Med J 2013;30(7):521-6. https://doi.org/10.1136/emermed-2012-201652
- Stone BA. Ultrasound guidance for peripheral venous access: a simplified seldinger technique. Anesthesiology 2007;106(1):195. https://doi.org/10.1097/00000542-200701000-00035
- Mahler SA, Wang H, Lester C, et al. Ultrasound-guided peripheral intravenous access in the emergency department using a modified Seldinger technique. J Emerg Med 2010;39(3):325-9. https://doi.org/10.1016/j.jemermed.2009.02.013
- Mills CN, Liebmann O, Stone MB, et al. Ultrasonographically guided insertion of a 15-cm catheter into the deep brachial or basilic vein in patients with difficult intravenous access. Ann Emerg Med 2007;50(1):68-72. https://doi.org/10.1016/j.annemergmed.2007.02.003
- Greca A, Iacobone E, Elisei D, et al. ECHOTIP: a structured protocol for ultrasound-based tip navigation and tip location during placement of central venous access devices in adult patients. J Vasc Access 2023;24(4):535-44. https://doi.org/10.1177/11297298211044325
- Zito MG, Biasucci DG, Barone G, et al. ECHOTIP-Ped: a structured protocol for ultrasound-based tip navigation and tip location during placement of central venous access devices in pediatric patients. J Vasc Access 2023;24(1):5-13. https://doi.org/10.1177/11297298211031391
- Biasucci DG. Ultrasound-based innovations for interventional procedures: the paradigmatic case of central venous access. Minerva Anestesiol 2020;86(2):121-3. https://doi.org/10.23736/S0375-9393.19
- Biasucci DG, La Greca A, Scoppettuolo G, et al. What’s really new in the field of vascular access? Towards a global use of ultrasound. Intensive Care Med 2015;41(4):731-3.https://doi.org/10.1007/s00134-015-3728-y
- Pittiruti M, Scoppettuolo G, Dolcetti L, et al. Clinical use of Sherlock-3CG® for positioning peripherally inserted central catheters. J Vasc Access 2019;20(4):356-61.https://doi.org/10.1177/1129729818805957
- Bedel J, Vallée F, Mari A, et al. Guidewire localization by transthoracic echocardiography during central venous catheter insertion: a periprocedural method to evaluate catheter placement. Intensive Care Med 2013;39(11):1932-7. https://doi.org/10.1007/s00134-013-3097-3
- .Zanobetti M, Coppa A, Bulletti F, et al. Verification of correct central venous catheter placement in the emergency department: comparison between ultrasonography and chest radiography. Intern Emerg Med 2013;8(2):173-80. https://doi.org/10.1007/s11739-012-0885-7
- Kim SC, Heinze I, Schmiedel A, et al. Ultrasound confirmation of central venous catheter position via a right supraclavicular fossa view using a microconvex probe: an observational pilot study. Eur J Anaesthesiol 2015;32(1):29-36. https://doi.org/10.1097/EJA.0000000000000042
- Kim SC, Gräff I, Sommer A, et al. Ultrasound-guided supraclavicular central venous catheter tip positioning via the right subclavian vein using a microconvex probe. J Vasc Access2016;17(5):435-9. https://doi.org/10.5301/jva.5000518
- Wang L, Liu ZS, Wang CA. Malposition of central venous catheter: presentation and management. Chin Med J (Engl) 2016;129(2):227-34. https://doi.org/10.4103/0366-6999.173525
- Lamperti M, Pittiruti M. Central venous catheter tip position: another point of view. Eur J Anaesthesiol 2015;32(1):3-4. https://doi.org/10.1097/EJA.0000000000000050
- Lamperti M, Bodenham AR, Pittiruti M, et al. International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med 2012;38(7):1105-17. https://doi.org/10.1007/s00134-012-2597-x
- Nakamuta S, Nishizawa T, Matsuhashi S, et al. Real-time ultrasound-guided placement of peripherally inserted central venous catheter without fluoroscopy. J Vasc Access2018;19(6):609-14. https://doi.org/10.1177/1129729818765057
- Matsushima K, Frankel HL. Bedside ultrasound can safely eliminate the need for chest radiographs after central venous catheter placement: CVC sono in the surgical ICU (SICU). J Surg Res 2010;163(1):155-61. https://doi.org/10.1016/j.jss.2010.04.020
- Maury E, Guglielminotti J, Alzieu M, et al. Ultrasonic examination: an alternative to chest radiography after central venous catheter insertion? Am J Respir Crit Care Med2001;164(3):403-5. https://doi.org/10.1164/ajrccm.164.3.2009042
- Miccini M, Cassini D, Gregori M, Gazzanelli S, Cassibba S, Biacchi D. Ultrasound-Guided Placement of Central Venous Port Systems via the Right Internal Jugular Vein: Are Chest X-Ray and/or Fluoroscopy Needed to Confirm the Correct Placement of the Device? World J Surg. 2016 Oct;40(10):2353-8. doi: 10.1007/s00268-016-3574-2. PMID: 27216807.
- Arellano R, Nurmohamed A, Rumman A, et al. The utility of transthoracic echocardiography to confirm central line placement: an observational study. Can J Anaesth 2014;61(4):340-6. https://doi.org/10.1007/s12630-014-0111-3. Erratum in: Can J Anaesth 2014;61(5):506.
- Vezzani A, Manca T, Vercelli A, et al. Ultrasonography as a guide during vascular access procedures and in the diagnosis of complications. J Ultrasound 2013;16(4):161-70. https://doi.org/10.1007/s40477-013-0046-5
- Vezzani A, Brusasco C, Palermo S, et al. Ultrasound localization of central vein catheter and detection of postprocedural pneumothorax: an alternative to chest radiography. Crit Care Med2010;38(2):533-8. https://doi.org/10.1097/CCM.0b013e3181c0328f
- Meggiolaro M, Scatto A, Zorzi A, et al. Confirmation of correct central venous catheter position in the preoperative setting by echocardiographic “bubble-test.” Minerva Anestesiol2015;81(9):989-1000.
- Ablordeppey EA, Drewry AM, Beyer AB, et al. Diagnostic accuracy of central venous catheter confirmation by bedside ultrasound versus chest radiography in critically ill patients: a systematic review and meta-analysis. Crit Care Med 2017;45(4):715-24. https://doi.org/10.1097/CCM.0000000000002188
- Smit JM, Raadsen R, Blans MJ, et al. Bedside ultrasound to detect central venous catheter misplacement and associated iatrogenic complications: a systematic review and meta-analysis. Crit Care 2018;22(1):65. https://doi.org/10.1186/s13054-018-1989-x
- Wen M, Stock K, Heemann U, et al. Agitated saline bubble-enhanced transthoracic echocardiography: a novel method to visualize the position of central venous catheter. Crit Care Med 2014;42(3):e231-3. https://doi.org/10.1097/CCM.0000000000000130
- Baviskar AS, Khatib KI, Bhoi S, et al. Confirmation of endovenous placement of central catheter using the ultrasonographic “bubble test”. Indian J Crit Care Med 2015;19(1):38-41. https://doi.org/10.4103/0972-5229.148642
- Pittiruti M, Scoppettuolo G. The GAVeCeLT Manual of PICC and Midline: Indications, Insertion, Management. Milan, Italy: Edra; 2017.
- Mantha SS, Kaushik PH, Nair AS, et al. Placement of tunneled peripherally inserted central catheter in femoral vein in a patient with major vessel thrombosis of upper extremity venous access for long-term chemotherapy. CHRISMED J Health Res 2021;8:134-5. https://doi.org/10.4103/cjhr.cjhr_56_19
- Naik VM, Cheruku DR, Swathi U, et al. Femoral peripherally inserted central catheter in superior vena cava syndrome – challenges of tunneling. Indian J Anaesth 2022;66(5):388-9. https://doi.org/10.4103/ija.ija_476_21
- Pinelli F, Pittiruti M, Van Boxtel T, et al. GAVeCeLT-WoCoVA consensus on subcutaneously anchored securement devices for the securement of venous catheters: current evidence and recommendations for future research. J Vasc Access 2021;22(5):716-25. https://doi.org/10.1177/1129729820924568
- Brescia F, Pittiruti M, Roveredo L, et al. Subcutaneously anchored securement for peripherally inserted central catheters: immediate, early, and late complications. J Vasc Access 2023;24(1):82-6. https://doi.org/10.1177/11297298211025430
- Rowe MS, Arnold K, Spencer TR. Catheter securement impact on PICC-related CLABSI: a university hospital perspective. Am J Infect Control 2020;48(12):1497-1500. https://doi.org/10.1016/j.ajic.2020.06
- Gekle R, Dubensky L, Haddad S, et al. Saline flush test: can bedside sonography replace conventional radiography for confirmation of above-the-diaphragm central venous catheter placement? J Ultrasound Med 2015;34(7):1295-9.https://doi.org/10.7863/ultra.34.7.1295
- Iacobone E, Elisei D, Gattari D, et al. Transthoracic echocardiography as bedside technique to verify tip location of central venous catheters in patients with atrial arrhythmia. J Vasc Access2020;21(6):861-7. https://doi.org/10.1177/1129729820905200
- Pittiruti M, Pelagatti F, Pinelli F. Intracavitary electrocardiography for tip location during central venous catheterization: a narrative review of 70 years of clinical studies. J Vasc Access2021;22(5):778-85. https://doi.org/10.1177/1129729820929835
- Calabrese M, Montini L, Arlotta G, et al. A modified intracavitary electrocardiographic method for detecting the location of the tip of central venous catheters in atrial fibrillation patients. J Vasc Access 2019;20(5):516-23. https://doi.org/10.1177/1129729818819422
- Wang D, Niu F, Gao H, et al. Influence of guide wire removal on tip location in peripherally inserted central catheters (PICCs): a retrospective cross-sectional study. BMJ Open2019;9(10):e027278. https://doi.org/10.1136/bmjopen-2018-027278
- Cho Y, Lee S, Park SJ, et al. Validation of the PICC length prediction formula based on anteroposterior chest radiographs for bedside ultrasound-guided placement. PLoS One2022;17(11):e0277526. https://doi.org/10.1371/journal.pone.0277526
- Russell E, Chan RJ, Marsh N, et al. A point prevalence study of cancer nursing practices for managing intravascular devices in an Australian tertiary cancer center. Eur J Oncol Nurs2014;18(3):231-5. https://doi.org/10.1016/j.ejon.2013.11.010
- Ullman AJ, Cooke ML, Mitchell M, et al. Dressings and securement devices for central venous catheters (CVC). Cochrane Database Syst Rev 2015;2015(9):CD010367. https://doi.org/10.1002/14651858.CD010367.pub2
- Ostroff MD, Moureau N, Pittiruti M. Rapid assessment of vascular exit site and tunneling options (RAVESTO): A new decision tool in the management of the complex vascular access patients. J Vasc Access 2023;24(2):311-7. https://doi.org/10.1177/11297298211034306
- Duran-Gehring PE, Guirgis FW, McKee KC, et al. The bubble study: ultrasound confirmation of central venous catheter placement. Am J Emerg Med 2015;33(3):315-9. https://doi.org/10.1016/j.ajem.2014.10.010
- Ostroff MD, Moureau NL. Report of modification for peripherally inserted central catheter placement: subcutaneous needle tunnel for high upper arm placement. J Infus Nurs2017;40(4):232-7. https://doi.org/10.1097/NAN.0000000000000228
- Chau A, Hernandez JA, Pimpalwar S, et al. Equivalent success and complication rates of tunneled common femoral venous catheter placed in the interventional suite vs. at patient bedside. Pediatr Radiol 2018;48(6):889-94. https://doi.org/10.1007/s00247-018-4090-3
- Pittiruti M, Pinelli F. GAVeCeLT working group for vascular access in COVID-19. Recommendations for the use of vascular access in the COVID-19 patients: an Italian perspective. Crit Care 2020;24(1):269. https://doi.org/10.1186/s13054-020-02997-1
- Giustivi D, Gidaro A, Baroni M, et al. Tunneling technique of PICCs and midline catheters. J Vasc Access 2022;23(4):610-14. https://doi.org/10.1177/11297298211002579
- S, Lucchini A. “Extended subcutaneous route” technique: a quick subcutaneous tunneling technique for PICC insertion. J Vasc Access 2017;18(3):269-72.https://doi.org/10.5301/jva.5000647
- Scoppettuolo G, Dolcetti L, Emoli A, et al. Further benefits of cyanoacrylate glue for central venous catheterisation. Anaesthesia 2015;70(6):758. https://doi.org/10.1111/anae.13105
- Zhang S, Guido AR, Jones RG, et al. Experimental study on the hemostatic effect of cyanoacrylate intended for catheter securement. J Vasc Access 2019;20(1):79-86. https://doi.org/10.1177/1129729818779702
- Nicholson J, Hill J. Cyanoacrylate tissue adhesive: a new tool for the vascular access toolbox. Br J Nurs 2019;28(19):S22-8. https://doi.org/10.12968/bjon.2019.28.19.S22
- Waller SC, Anderson DW, Kane BJ, et al. In vitro assessment of microbial barrier properties of cyanoacrylate tissue adhesives and pressure-sensitive adhesives. Surg Infect (Larchmt) 2019;20(6):449-52. https://doi.org/10.1089/sur.2018.280
- Ostroff M, Zauk A, Chowdhury S, et al. A retrospective analysis of the clinical effectiveness of subcutaneously tunneled femoral vein cannulations at the bedside: a low risk central venous access approach in the neonatal intensive care unit. J Vasc Access2021;22(6):926-34. https://doi.org/10.1177/1129729820969291
- Bertoglio S. Reverse tapered versus non-tapered peripherally inserted central catheters: a narrative review. J Vasc Access 2022;23(5):689-91. https://doi.org/10.1177/11297298211009998
- Bainbridge P, Browning P, Bernatchez SF, et al. Comparing test methods for moisture-vapor transmission rate (MVTR) for vascular access transparent semipermeable dressings. J Vasc Access 2021;24(5):11297298211050485. https://doi.org/10.1177/11297298211050485
- Hoffmann KK, Weber DJ, Samsa GP, et al. Transparent polyurethane film as an intravenous catheter dressing. A meta-analysis of the infection risks. JAMA1992;267(15):2072-6.
- Maki DG, Ringer M. Evaluation of dressing regimens for prevention of infection with peripheral intravenous catheters. Gauze, a transparent polyurethane dressing, and an iodophor-transparent dressing. JAMA 1987;258(17):2396-403.
- Webster J, Gillies D, O’Riordan E, et al. Gauze and tape and transparent polyurethane dressings for central venous catheters. Cochrane Database Syst Rev 2011;(11):CD003827.https://doi.org/10.1002/14651858.CD003827.pub2 Update in: Cochrane Database Syst Rev2016;(5):CD003827. https://doi.org/10.1002/14651858.CD003827.pub3
- O’Grady NP, Alexander M, Burns LA,et al. Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 2011;52(9):e162-93. https://doi.org/10.1093/cid/cir257
- Teichgräber UK, de Bucourt M, Gebauer B, et al. Effectiveness of sutureless percutaneous placement of cuffed tunneled hemodialysis catheters applying StatLock attachment devices. J Vasc Access 2011;12(1):17-20. https://doi.org/10.5301/jva.2010.6089
- Amerasekera SS, Jones CM, Patel R, et al. Imaging of the complications of peripherally inserted central venous catheters. Clin Radiol 2009;64(8):832-40. https://doi.org/10.1016/j.crad.2009.02.021
- Rowley S, Clare S, Macqueen S, et al. ANTT v2: An updated practice framework for aseptic technique. Br J Nurs 2010;195):S5-11. https://doi.org/10.12968/bjon.2010.19.Sup1.47079
- Haller LT, Rush KL. Central line infection: a review. J Clin Nurs 1992;1:61-6.
- Meng Hu, Zhi-Cheng Ma, Jie Zhang, et al. A peripherally inserted central vein catheter fractured and slid into the right pulmonary artery: a case report. Chinese Nursing Research 2–3,2015;2(2-3): 86-8. https://doi.org/10.1016/j.cnre.2015.09.005
- Zhong L, Wang HL, Xu B, et al. Normal saline versus heparin for patency of central venous catheters in adult patients – a systematic review and meta-analysis. Crit Care2017;21(1):5. https://doi.org/10.1186/s13054-016-1585-x
- Hadaway L. Technology of flushing vascular access devices. J Infus Nurs2006;29(3):137-45. https://doi.org/10.1097/00129804-200605000-00003
- Cotogni P, Pittiruti M. Focus on peripherally inserted central catheters in critically ill patients. World J Crit Care Med 2014;3(4):80-94. https://doi.org/10.5492/wjccm.v3.i4.80
- Pittiruti M, Hamilton H, Biffi R, et al. ESPEN guidelines on parenteral nutrition: central venous catheters (access, care, diagnosis and therapy of complications). Clin Nutr2009;28(4):365-77. https://doi.org/10.1016/j.clnu.2009.03.015
- Smith RJ, Cartin-Ceba R, Colquist JA, et al. Peripherally inserted central catheter placement in a multidisciplinary intensive care unit: a preliminary study demonstrating safety and procedural time in critically ill subjects. J Vasc Access 2021;22(1):101-6. https://doi.org/10.1177/1129729820928618
- Gupta N, Gandhi D, Sharma S, et al. Tunneled and routine peripherally inserted central catheters placement in adult and pediatric population: review, technical feasibility, and troubleshooting. Quant Imaging Med Surg 2021;11(4):1619-27. https://doi.org/10.21037/qims-20-694
- Krein SL, Saint S, Trautner BW, et al. Patient-reported complications related to peripherally inserted central catheters: a multicentre prospective cohort study. BMJ Qual Saf2019;28(7):574-81. https://doi.org/10.1136/bmjqs-2018-008726
- White D, Woller SC, Stevens SM, et al. Comparative thrombosis risk of vascular access devices among critically ill medical patients. Thromb Res 2018;172:54-60. https://doi.org/10.1016/j.thromres.2018.10.013
- Menéndez JJ, Verdú C, Calderón B, et al. Incidence and risk factors of superficial and deep vein thrombosis associated with peripherally inserted central catheters in children. J Thromb Haemost 2016;14(11):2158-68. https://doi.org/10.1111/jth.13478
- Moureau N, Lamperti M, Kelly LJ, et al. Evidence-based consensus on the insertion of central venous access devices: definition of minimal requirements for training. Br J Anaesth2013;110(3):347-56. https://doi.org/10.1093/bja/aes499
- Moran J, Colbert CY, Song J, et al. Screening for novel risk factors related to peripherally inserted central catheter-associated complications. J Hosp Med 2014;9(8):481-9. https://doi.org/10.1002/jhm.2207
- Walz JM, Memtsoudis SG, Heard SO. Prevention of central venous catheter bloodstream infections. J Intensive Care Med 2010;25(3):131-8. https://doi.org/10.1177/0885066609358952
- Babu MSS, Gadhinglajkar SV, Gayathri G, et al. Role of ultrasound imaging of subclavian vein to confirm correct placement of the peripheral intravenous cannula to avoid extravasation in an edematous patient. J Anaesthesiol Clin Pharmacol 2025;41(4):742-3. https://doi.org/10.4103/joacp.joacp_406_24