How I Do It: X-Ray-Guided Cervical Nerve Root Block via the Posterolateral Oblique Approach
Cite as: Nakamura H, Hashizume K, Yamagami H. How I do it: x-ray-guided cervical nerve root block via the posterolateral oblique approach. ASRA Pain Medicine News 2026;51. https://doi.org/10.52211/asra050126.011.
How I Do It
Introduction
Selective cervical nerve root block (SCNRB) is a commonly performed procedure to alleviate pain from a variety of causes of cervical radiculopathy, such as intervertebral disc herniation, spondylosis, spinal canal stenosis, and herpes zoster-associated pain.1
There are several approaches for SCNRB, including the anterolateral and posterolateral approaches (Figure 1). The anterolateral approach is widely used, but because the needle advances directly into the intervertebral foramen (IVF), there is a risk of spinal canal invasion and vascular puncture.2,3 The posterolateral approach, on the other hand, is difficult to perform with fluoroscopy alone. It has been performed under CT guidance4,5 and, more recently, with ultrasound guidance.6,7 With both CT and ultrasound guidance, it’s expected that the needle won’t easily reach the deep area of the IVF, leading to fewer complications.
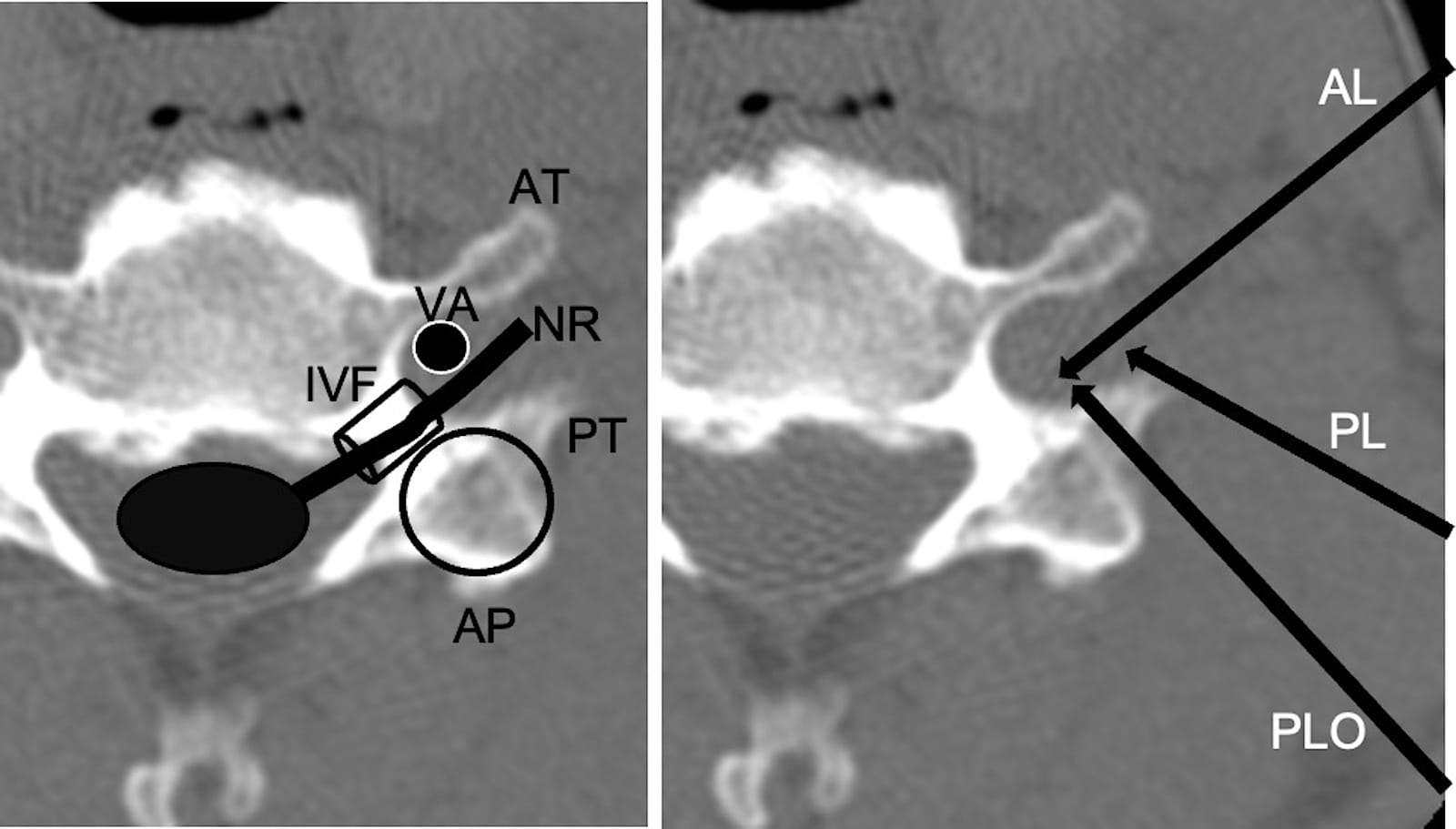
Figure 1. Approaches for cervical nerve root blocks.
Left panel: This image shows the anatomy of a C6 vertebra on an axial CT scan. The circle represents the articular pillar (AP). Other labeled structures include the anterior tubercle (AT), posterior tubercle (PT), nerve root (NR), and vertebral artery (VA). The tube-shaped structure is the intervertebral foramen (IVF) tunnel.
Right panel: This image illustrates the approaches for cervical nerve root blocks. AL stands for the anterolateral approach, PL for the posterolateral approach (under ultrasound guidance), and PLO for the posterolateral oblique approach (our procedure).
In this discussion, we describe a “posterolateral oblique approach” for performing SCNRBs under fluoroscopic guidance, as first reported in Japanese by Yamagami et al. (Pain-Clinic 1993;14:591-4) and further detailed by Hashizume et al.8 A key feature of this technique is that the needle is initially guided to the superior articular process (SAP). The needle then maintains contact with the articular pillar, sliding along it until the tip reaches the inter-tuberculous sulcus, which is the outlet of the IVF (Figure 1). By using the articular pillar to restrict the needle’s trajectory, we believe we can minimize the risk of accidental deep entry into the IVF and precisely reach the nerve root at the outlet of the IVF tunnel.
Anatomy
The nerve roots from C3 to C6 exit the IVFs, pass through the sulcus between the anterior and posterior tubercles, and travel laterally.9 The C7 nerve root has no anterior tubercle and passes along the anterior surface of the posterior tubercle. The C8 nerve root passes through the space between the caudal side of the C7 posterior tubercle and the cranial side of the first rib base. The depth of the inter-tuberculous sulcus is shallow at C3 and C4, but becomes deeper from C5 onward. Additionally, the height of the posterior tubercle relative to the anterior tubercle also increases from C5 onward (Figure 2).
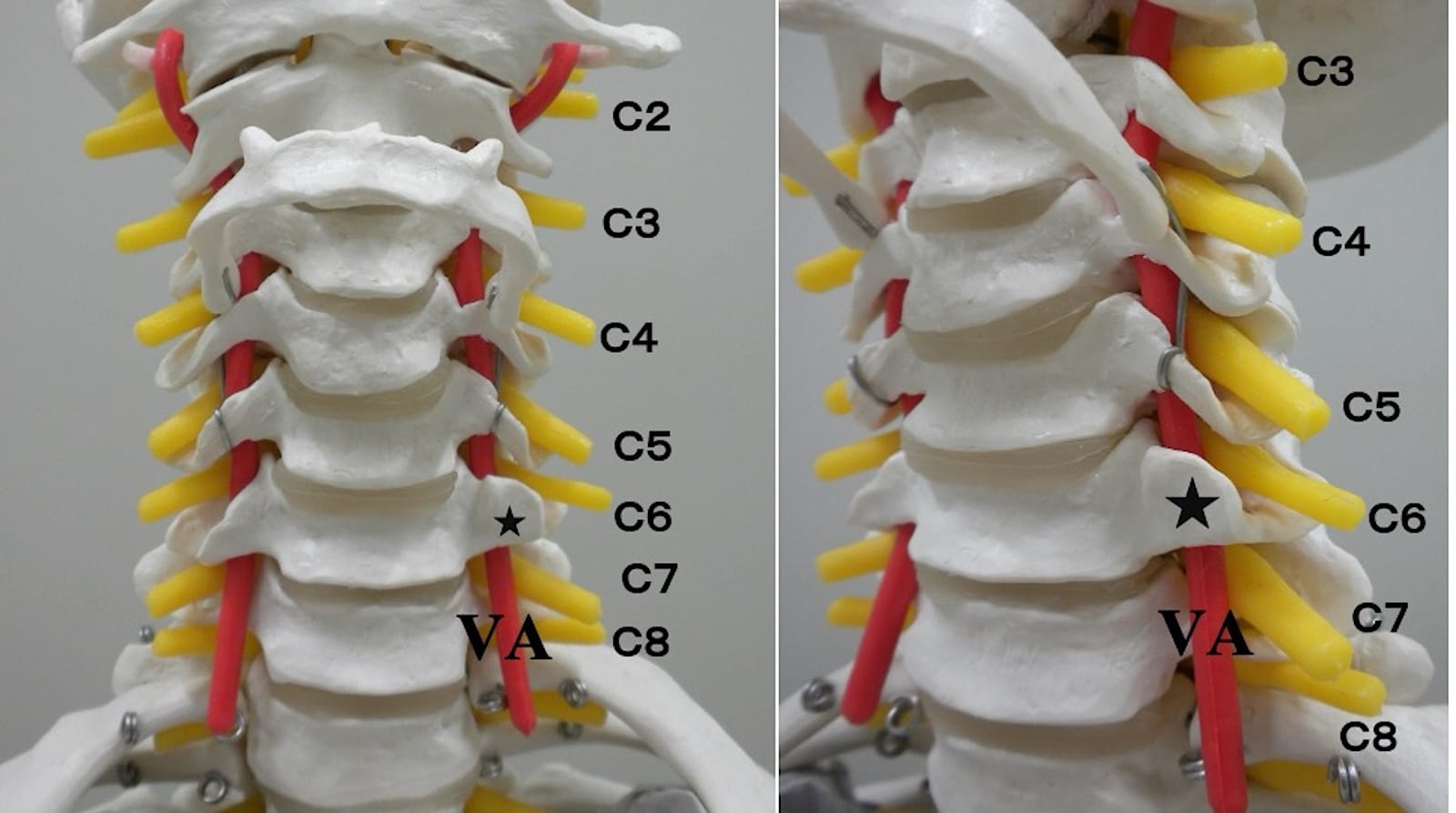
Figure 2. Cervical vertebra, nerve, and vertebral artery.
These are the frontal (left) and oblique (right) cervical spine models. Each nerve root exits from an intervertebral foramen and runs through the intertuberculous sulcus. The star indicates the anterior tubercle of C6. C7, located below C6, has no anterior tubercle. The vertebral artery passes through the transverse foramen of the C6 vertebra and ascends along the ventral side of each nerve root.
Star mark = anterior tubercle of C6, C2-C8= C2-C8 nerve roots, VA = vertebral artery.
Generally, the vertebral artery (VA), which branches from the subclavian artery, passes through the transverse foramen of the C6 vertebra, continues through the transverse foramina of each cervical vertebra, ascends along the ventral side of the nerve roots, and enters the cranium through the foramen magnum.3 Branches of the VA (radicular arteries) and branches from the ascending cervical artery or deep cervical artery (segmental arteries) run parallel most frequently to the superoventral side of the nerve roots as they head into the spinal canal from the IVF.10 Some of these arteries reach the spinal cord and join the anterior and posterior spinal arteries. Furthermore, various anatomical variants of the VA have been documented. The VA may enter the transverse foramen at levels other than C6,11 with entries at C5, C4, or C7 being the most frequent; in such cases, the VA diameter on the anomalous side is often smaller than that on the contralateral side.12
X-ray-guided cervical nerve root block via the posterolateral oblique approach is a valuable and precise technique for managing cervical radiculopathy.
These entry levels are reported to correlate embryologically with variations in the VA origin; most commonly, a VA originating more proximally (closer to the heart) tends to enter the transverse foramen at the C5 level.13 Additionally, morphological anomalies of the cervical vertebrae, such as the presence of a duplicate transverse foramen, are frequently associated with anomalous VA configurations.14 As cervical spondylosis progresses, the VA may become closer to the IVF.15 An abundant venous plexus is also present around the IVF. Given these anatomical complexities, clinicians must always remain vigilant for potential variations in cervical morphology and VA course when performing nerve blocks. In cases where such anomalies are suspected, pre-procedural CT angiography should be considered to ensure safety.
How to Match Body Position and Fluoroscopy
The patient is positioned in a lateral decubitus position with the affected side up. A high pillow is used to ensure the spinal axis is perpendicular to the line of the shoulders. Tilting the fluoroscope axis 20-30 degrees caudally from vertical improves visibility of the IVFs (Figure 3A). When the patient is tilted 45 degrees dorsally from vertical, an oblique view shows the IVFs in full view. In our clinical practice, the patient is tilted slightly dorsally, 20-30 degrees from the vertical, to adjust the view so that the SAP superimposes the dorsal third of the IVF (Figure 3B). This semi-oblique view prepares for the “posterolateral oblique approach.” This view allows us to clearly visualize the SAP's shape, which is the initial target for the needle.
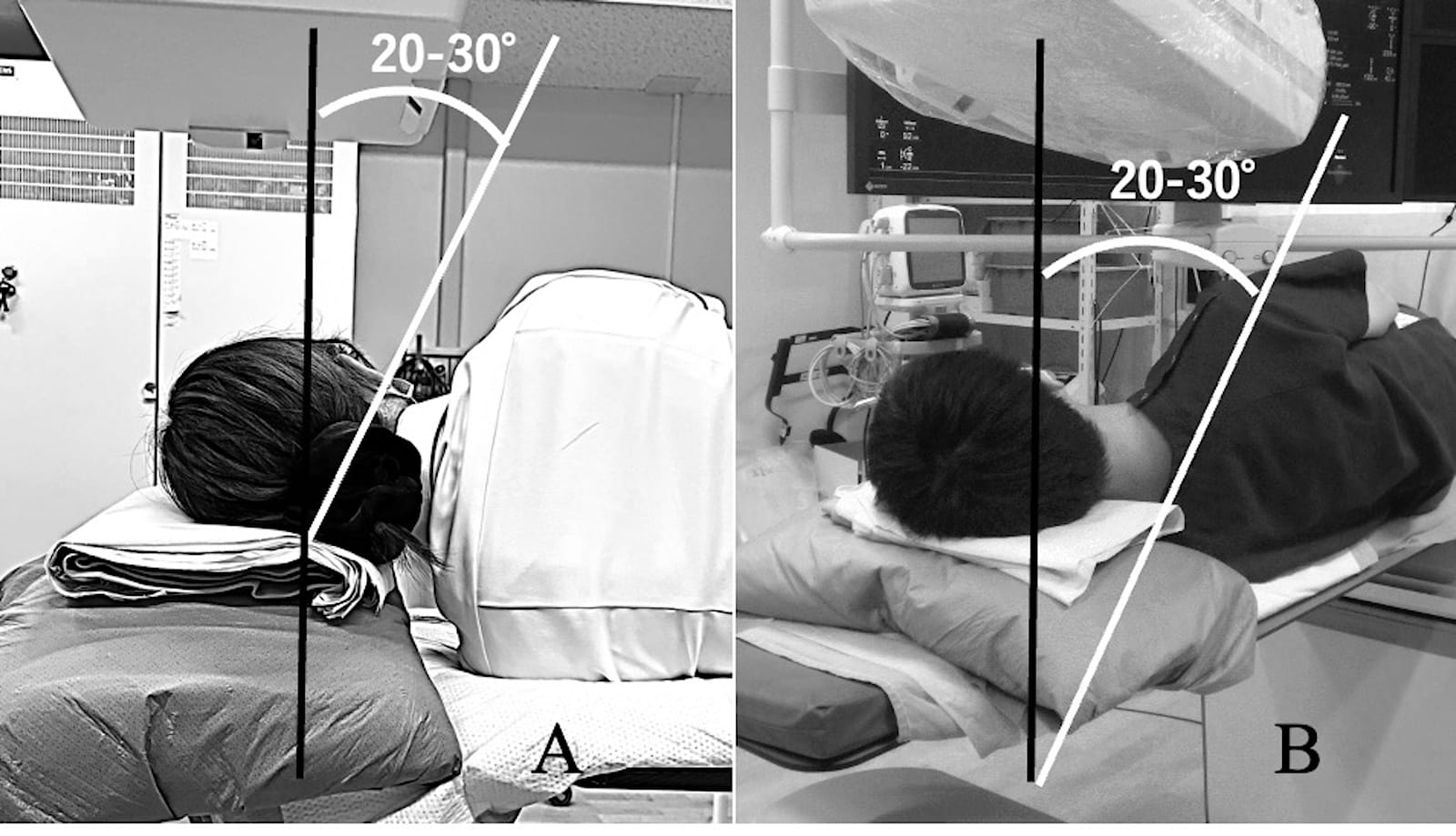
Figure 3. The setting of body position and the axis of the fluoroscope.
(A) Use a high pillow and pull the patient’s lower arm caudally to ensure the spinal axis is perpendicular to the line of the shoulders. The axis of the fluoroscopy (white line) is tilted 20-30 degrees caudally from the vertical to clearly see the intervertebral foramen.
(B) The white line indicates the line between the shoulders. Tilt the patient 20-30 degrees dorsally from the vertical to create a semi-oblique view in preparation for a posterolateral oblique approach.
Procedure
Equipment and Drugs
Needles: 25G or 23G 60-90 mm needles; local anesthetic: 1% mepivacaine; contrast agent: iohexol 240 mgI/mL; block agents: approximately 1 mL of 0.5% mepivacaine mixed with approximately 1 mg of dexamethasone (dexamethasone is available as 3.3 mg/mL in my hospital). The following disinfectants are required: 0.5% chlorhexidine + ethanol or povidone-iodine solution, cotton balls, gauze, Kocher forceps, and a drape.
Procedure Details
In the semi-oblique view, the needle insertion point is the tip of the spinous process of the cervical vertebra superior to the target nerve root. As described in the anatomy section, the lower the cervical vertebra, the more acute the angle required to avoid the posterior tubercle. Therefore, for C3 and C4, the needle is advanced horizontally, whereas for C5, C6, C7, and C8, the needle is inserted with a downward trajectory (Figures 4 and 5). After insertion, the needle is first brought into contact with the lateral wall of SAP.
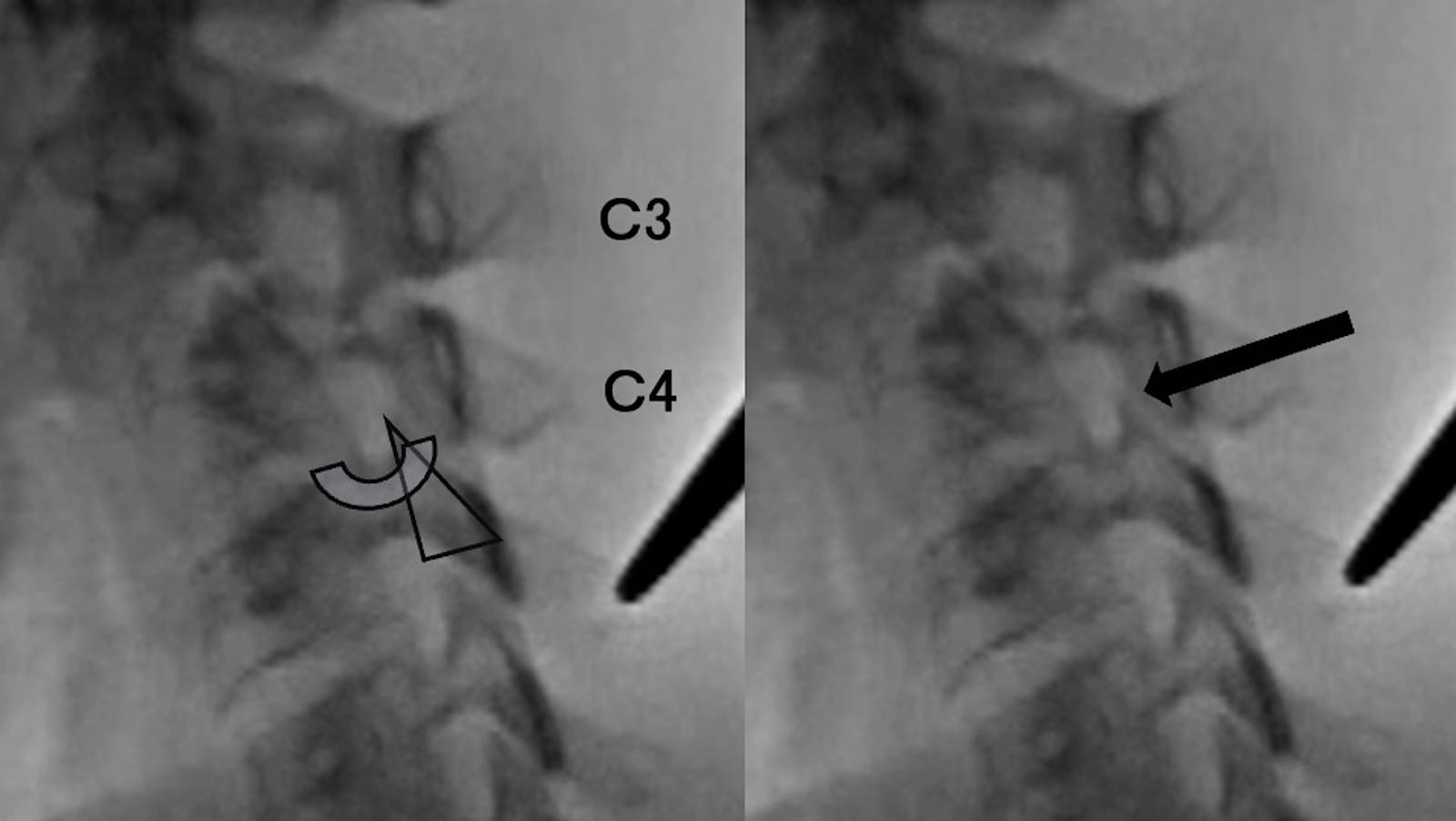
Figure 4. Needle insertion points and directions for C3 and C4.
The needle is advanced horizontally for C3 and C4 because their posterior tubercles are low.
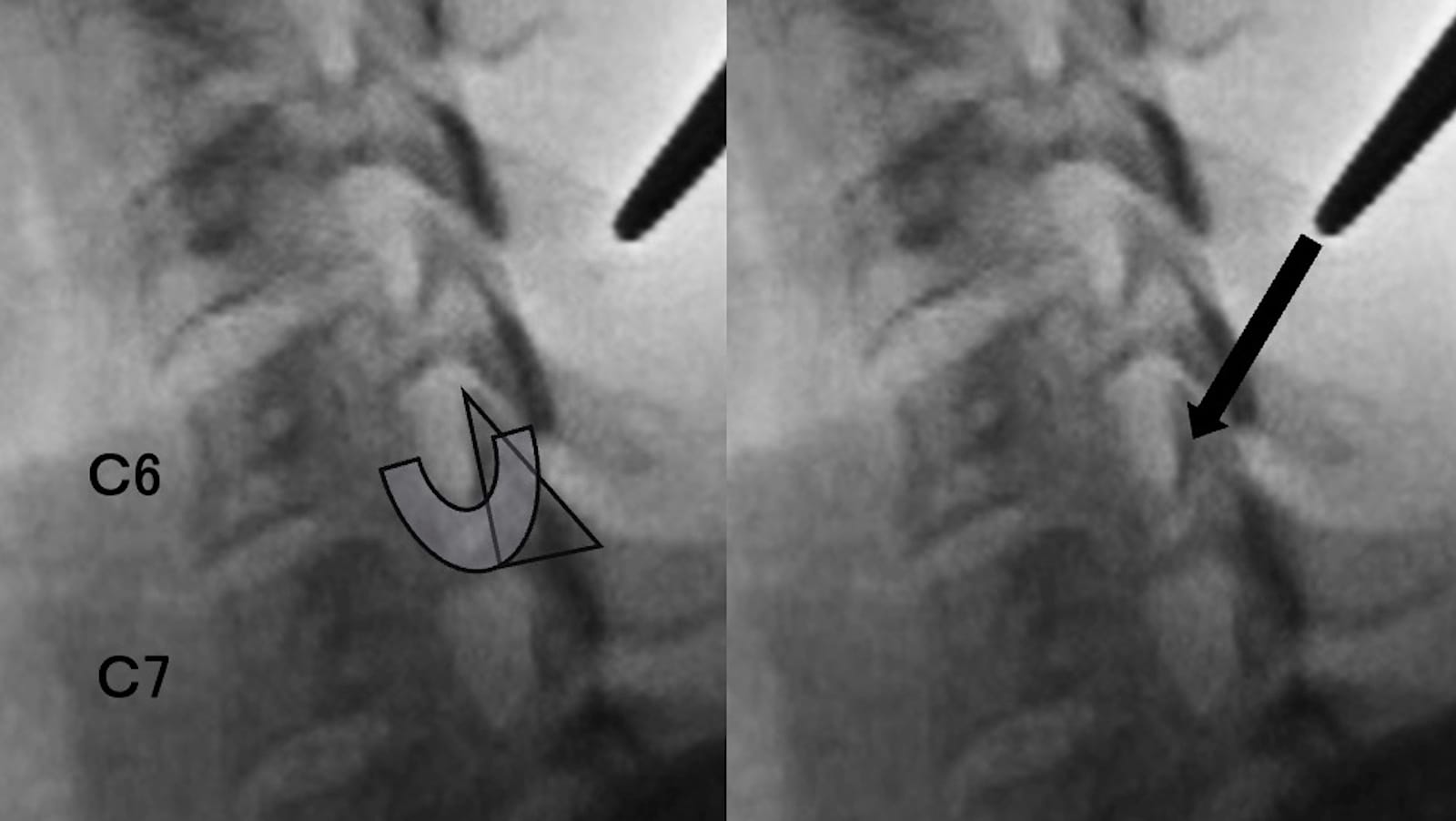
Figure 5. Needle insertion points and directions for C5-8.
As a more acute angle is required to avoid the high posterior tubercle in the lower cervical vertebrae, downward trajectories are necessary for C5, C6, C7, and C8.
Then, while maintaining contact with the articular pillar, the needle tip is slid into the lower half of the IVF (Figure 6, Video 1). At this time, it is crucial not to advance the needle too far into the ventral side of the inter-tuberculous sulcus, as the VA is located on the ventral side and the segmental and radicular arteries are on the superoventral side. To anticipate the risk of spinal canal invasion, the fluoroscope is rotated to the anteroposterior view to confirm that the needle tip has not advanced past the medial side of the articular pillar before proceeding with contrast injection.
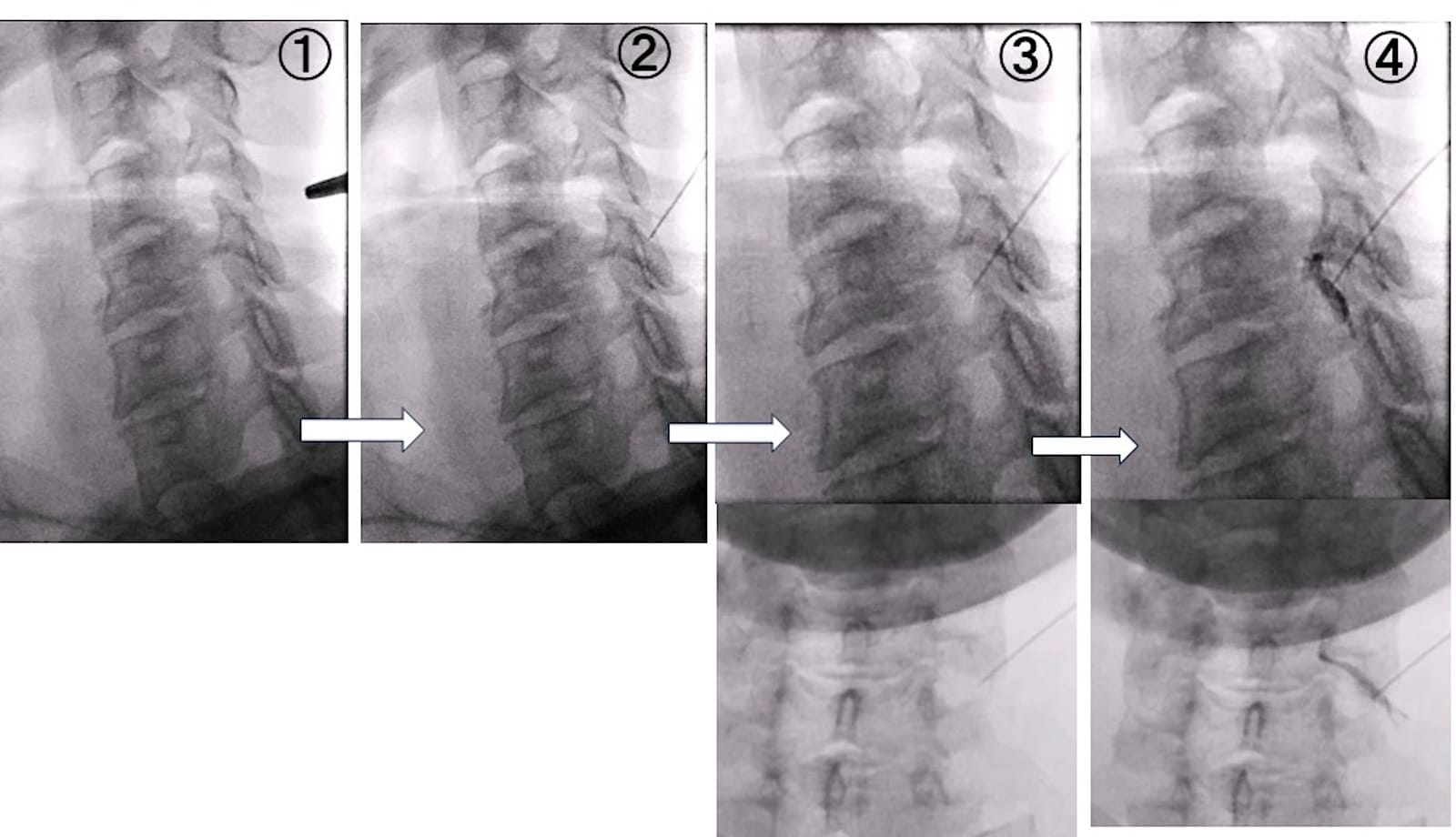
Figure 6. Left C6 cervical nerve root block using a posterolateral oblique approach.
① Hold the insertion point with forceps and insert the needle. ② Initially, bring the needle into contact with the superior articular process. ③ While maintaining contact with the articular pillar, slide the needle tip into the lower half of the intervertebral foramen. An AP view is also checked. The needle tip does not reach the midline of the articular pillar in the AP view. ④ Inject contrast, confirming that the intervertebral foramen is filled. Radiculography and a small amount of transforaminal epidural flow are also seen.
Video 1. X-Ray-guided cervical nerve root block (left C6) via the posterolateral oblique approach.
Points to Note and Clinical Pearls
- For a slender, thin neck, the needle is inserted closer to the articular pillar. For a thick neck with well-developed muscles, it is inserted closer to the tip of the spinous process; in other words, for a thicker neck, the entry point is more dorsal.
- Since the skin is thin, it can easily shift under the needle puncture, causing it to deviate from the intended insertion pathway. Adjustments should be made while the needle tip is still just under the skin. It is important to maintain the intended needle pathway from the beginning to the end of the procedure.
Interpretation of Contrast and Injection of Drugs
A small amount of contrast agent, approximately 0.5 to 2 mL, should be injected slowly. The success of the block is confirmed by visualizing the contrast collection over the IVF on the lateral view; a frontal view should also be checked. The result of the contrast injection is typically a perineural spread, sometimes accompanied by a transforaminal epidural contrast effect (Figure 6, Video 1). If the image is appropriate, approximately 1 mL of 0.5% mepivacaine mixed with approximately 1mg of dexamethasone should be injected. The dose should be adjusted based on the patient. After the nerve block, vital signs should be monitored, and bed rest should be maintained for at least 45 minutes.
Points to Note and Clinical Pearls
- Pain may not be reported with a spinal puncture alone, but injecting a contrast agent into the spinal cord can cause severe pain and lead to neurological damage. The depth of the needle cannot be determined on the lateral view. To avoid injury to the spinal cord, the tip of the needle should not pass the midline of the articular pillar on the frontal view. We caution against injecting contrast without checking the AP view.
- The needle position can easily shift when switching the syringe. To maintain stability during the procedure, it’s best to use a connecting tube between the needle and the syringe.
- Contrast spread into the facet joint sometimes occurs more frequently in the upper cervical spine. In such cases, advancing the needle slightly further often reaches the intervertebral foramen.
- Vascular injections can be observed simultaneously with nerve root contrast. If this occurs, you may withdraw the needle slightly and adjust its direction, but it is crucial not to force the injection if intravascular injection is unavoidable.
- Arterial injection is pulsatile. Radicular artery injection follows the nerve root into the spinal canal (Video 2), while VA injection moves in a cranial direction. Both disappear in an instant. A pulsatile contrast that disappears instantly warrants caution.
- Venous injection spreads slowly and irregularly in a spiderweb-like pattern around the intervertebral foramen and disappears slowly (Figure 7).
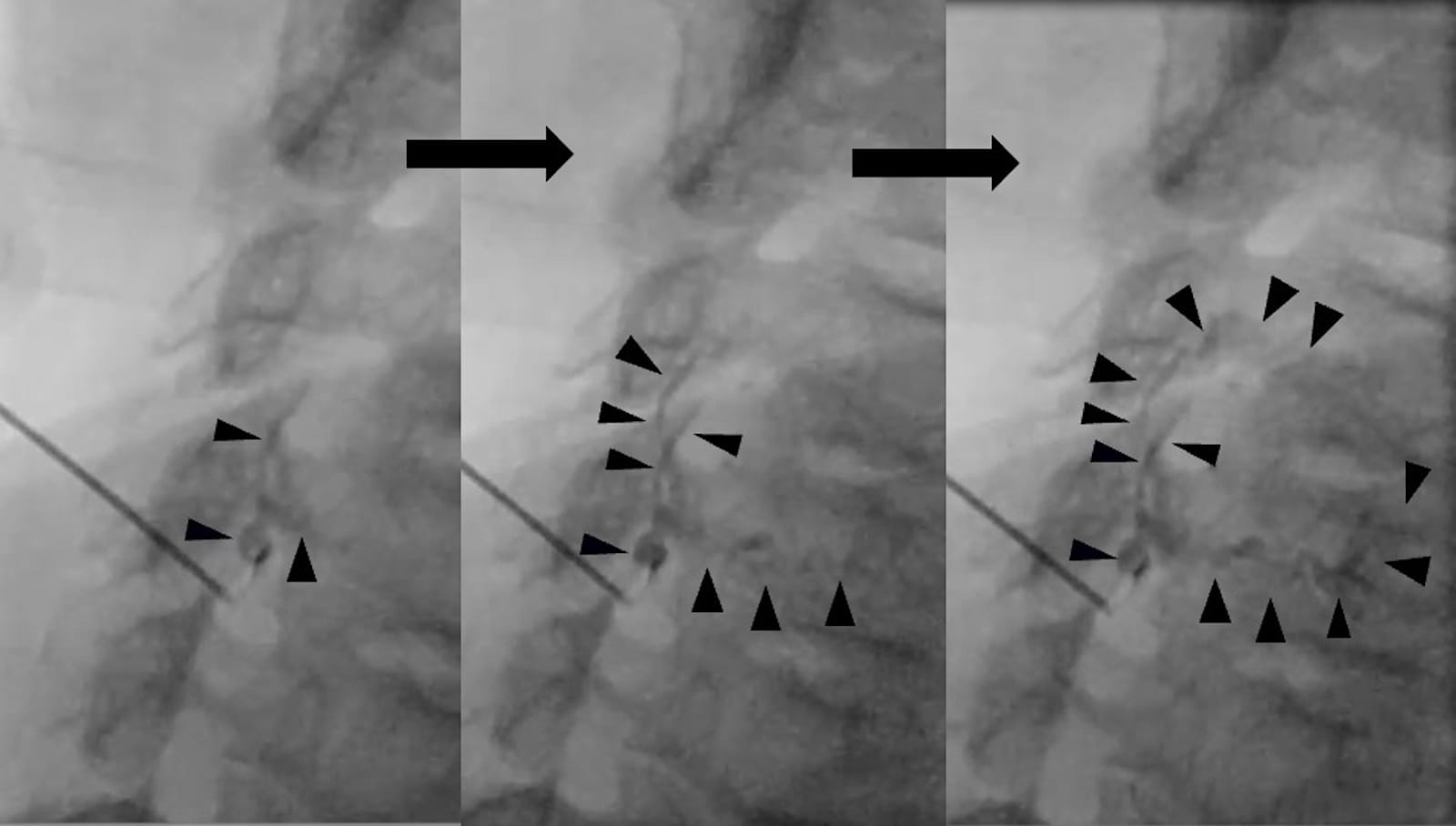
Figure 7. Venous contrast.
These images were captured as a continuous sequence during a right C6 nerve root block that lasted approximately 5 seconds. The contrast agent can be seen spreading into the venous plexus in a spiderweb-like pattern before slowly disappearing.
Black arrow = contrasted veins.
Modified from Hashizume K et al. Pain Res 2024;39:26-34.
Video 2. Accidental contrast injection into the radicular artery during a right C6 nerve root block.
Complications
Potential minor complications include subcutaneous hemorrhage, subcutaneous abscess, hypotension, malaise, and bradycardia. Potential major complications include subarachnoid injection leading to cardiac or respiratory arrest, postdural puncture headache, spinal cord injury, spinal ischemia due to inadvertent intra-arterial injection or arterial spasm, epidural hematoma due to vascular injury, epidural abscess, and myelitis.
Discussion
SCNRB using the posterolateral oblique approach is performed by first positioning the needle on the SAP and then sliding it along the bone surface to reach the outlet of the IVF. Contact with the SAP helps to prevent the needle from straying and maintains the intended pathway. A frontal view can also help prevent spinal cord injury. Using contrast agents allows for clear visualization of anatomical structures, ensuring accurate targeting of the nerve block and helping detect vascular injection early.
Based on anatomical considerations, to avoid vascular puncture during an SCNRB, it is important not to advance the needle to the cranioventral side of the IVF, where the radicular and segmental arteries often run, or to the ventral side beyond the IVF, where the VA runs.4,10 With the anterolateral approach, there is a risk of the needle entering too deeply into the IVF due to its trajectory. This could damage the arteries around the nerve root, lead to intra-arterial injection, or puncture the dura or spinal cord. There have been reports of complications, such as spinal cord infarction and spinal cord injury.16,17 In contrast, the posterolateral approach can more effectively anatomically avoid these critical structures than the anterolateral approach.18
Case reports describe the posterolateral approach using CT and ultrasound guidance.4,5 However, CT guidance presents a problem with radiation exposure. Our method using fluoroscopy leads to less radiation exposure than CT guidance. Ultrasound-guided cervical nerve root block, which aims posterolaterally for the inter-tuberculous sulcus, has the advantage of no radiation exposure and enables us to detect and avoid blood vessels on the tract of the needle.6,7 However, as discussed in the anatomy section, anatomical variants of the vasculature are often thinner than normal arteries. Visualizing these minute vessels—especially those adjacent to bone—can be challenging using ultrasound alone.19 This suggests that the adjunct use of fluoroscopy prior to the final drug injection may be a safer approach to ensure the absence of intravascular uptake. There are also reports of combining ultrasound-guided blocks with fluoroscopy.20
With ultrasound guidance, the needle often reaches the cervical nerve root at the intertubercular sulcus, which often generates contrast images of the brachial plexus.21 In comparison, with the posterolateral oblique approach, the needle advances while in contact with the articular pillar and reaches the outlet of the intervertebral foramen, which is more central than the intertuberculous sulcus.
/feathr-26-membership-and-edge-300x250-rev.jpg?sfvrsn=9211363d_1 "feathr 26 membership and EDGE 300x250 REV")
Conclusion
X-ray-guided cervical nerve root block via the posterolateral oblique approach is a valuable and precise technique for managing cervical radiculopathy. By enabling continuous needle visualization and anatomical confirmation with contrast agents, this method enhances targeting accuracy and early detection of complications, thereby offering an effective therapeutic option for pain management.

Hiroki Nakamura, MD, is a fellow physician at the Pain Center at Kouseikai Takai Hospital in Nara, Japan.

Keiji Hashizume, MD, PhD, is the director of the Pain Center at Kouseikai Takai Hospital in Nara, Japan.

Hiroaki Yamagami, MD, PhD, is the director of the Yamato Pain Clinic in Osaka, Japan.
References
- Borton ZM, Oakley BJ, Clamp JA, et al. Cervical transforaminal epidural steroid injections for radicular pain: a systematic review. Bone Joint J 2022;104: 567-74. https://doi.org/10.1302/0301-620X.104B5.BJJ-2021-1816.R1
- Otto FW, Pluhm R, Ozturk K, et al. Counterpoint: conventional fluoroscopy-guided selective cervical nerve root block- a safe, effective, and efficient modality in the hands of an experienced proceduralist. AJNR Am J Neuroradiol 2020;41:1112-9. https://doi.org/10.3174/ajnr.A6580
- Rathmell JP, Benzon HT, Dreyfuss P, et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology 2015; 122:974-84. https://doi.org/10.1097/ALN.0000000000000614
- Wald JT, Maus TP, Geske JR, et.al. Safety and efficacy of CT-guided transforaminal cervical epidural steroid injections using a posterior approach. AJNR Am J Neuroradiol 2012;33:415-19. https://doi.org/10.3174/ajnr.A2835
- Reddy S, Wu J. Extraforaminal cervical selective nerve root block-description of a posterolateral approach with cone beam-based CT guidance. Pain Pract 2020;20:919-28. https://doi.org/10.1111/papr.12923
- Cui X, Zhang D, Zhao Y, et al. An open-label non-inferiority randomized trial comparing the effectiveness and safety of ultrasound-guided selective cervical nerve root block and fluoroscopy-guided cervical transforaminal epidural block for cervical radiculopathy. Ann Med 2022;54:2681-91. https://doi.org/10.1080/07853890.2022.2124445
- Ehsanian R, Schneider BJ, Kennedy DJ, et al. Ultrasound-guided cervical selective nerve root injections: a narrative review of literature. Res Anesth Pain Med 2021;46:416-21. https://doi.org/10.1136/rapm-2020-102325
- Hashizume K, Yamagami H, Iwata T, et al. Outcomes of 707 cervical selective nerve root blocks using a fluoroscopy–guided posterolateral oblique approach. Pain Research 2024;39:26-34. https://doi.org/10.11154/pain.39.26
- Ebraheim NA, An HS, Xu R, et al. The quantitative anatomy of the cervical nerve root groove and the intervertebral foramen. Spine (Phila, Pa 1976). 1996;21:1619-23. https://doi.org/10.1097/00007632-199607150-00001
- Jun B, Yang HM, Shin DA, et al. Anatomical location of the segmental spinal arteries in the cervical intervertebral foramina: 3D-micro CT findings relevant to transforaminal epidural injection. J Pain Res 2025;18:701-8. https://doi.org/10.2147/JPR.S495046
- Eskander MS, Drew JM, Aubin ME, et al. Vertebral artery anatomy: a review of two hundred fifty magnetic resonance imaging scans. Spine (Phila, Pa 1976). 2010;35(23):2035-40. https://doi.org/10.1097/BRS.0b013e3181c9f3d4
- Kim JT, Lee HJ, Kim JH, et al. Quantitative analysis of unusual entrance of the vertebral artery into the cervical foramen (V2 segment) and its clinical implications. Eur Spine J 2016;25(12):4188-94. https://doi.org/10.1007/s00586-016-4708-9
- Bueno HF, Nimchinsky EA. Mapping of anatomic variants of the proximal vertebral artery in relation to embryology. AJNR Am J Neuroradiol 2023;44(8):943-50. https://doi.org/10.3174/ajnr.A7942
- Zibis A, Mitrousias V, Galanakis N, et al Variations of transverse foramina in cervical vertebrae: what happens to the vertebral artery? Eur Spine J 2018;27(6):1278-85. https://doi.org/10.1007/s00586-018-5523-2
- Fitzgerald RT, Bartynski WS, Collins HR. Vertebral artery position in the setting of cervical degenerative disease: implications for selective cervical transforaminal epidural injections. Interv Neuroradiol 2013;19:425-31. https://doi.org/10.1177/159101991301900404
- Benny B, Azari P, Briones D. Complications of cervical transforaminal epidural steroid injections. Am J Phys Med Rehabil 2010;89:601-7. https://doi.org/10.1097/PHM.0b013e3181e2d07c
- Scanlon GC, Moeller-Bertram T, Romanowsky SM, et al. Cervical transforaminal epidural steroid injections: more dangerous than we think? Spine 2007;32: 1249-56. https://doi.org/10.1097/BRS.0b013e318053ec50
- Wolter T, Mohadjer M, Berlis A, et al. Cervical CT-guided, selective nerve root blocks: improved safety by dorsal approach. Am J Neuroradiol 2009;30: 336-7. https://doi.org/10.3174/ajnr.A1222
- Lee HH, Park D, Oh Y, et. Ultrasonography evaluation of vulnerable vessels around cervical nerve roots during selective cervical nerve root block. Ann Rehabil Med 2017;41(1):66-71. https://doi.org/10.5535/arm.2017.41.1.66
- Wakeling C, Bateman A, Hatrick A, et al. Combined fluoroscopic and ultrasound guided cervical nerve root injections. Int Orthop 2016;40:2547-51. https://doi.org/10.1007/s00264-016-3224-1
- Falyar CR, Abercrombie C, Becker R, et al. Intrathecal spread of injectate following an ultrasound-guided selective C5 nerve root injection in a human cadaver model. AANA J 2016;84: 80-4.